Key learning points
At the end of this article, the reader will:
- •
Appreciate why bleeding is a problem in endoscopic sinus and skull base surgery.
- •
Understand the reasons for avoiding traditional nasal packing after endoscopic nasal surgery.
- •
Be familiar with the evolution of materials and devices in endoscopic sinus and skull base surgery.
- •
Be able to discuss the benefits and drawbacks of topical materials in use today.
- •
Be able to apply appropriate mechanisms to avoid bleeding in sinus and skull base surgery.
Introduction
Functional endoscopic sinus and skull base surgery has become an effective part of the management of chronic rhinosinusitis and tumors of the sinuses and anterior skull base. Technologic advances have been critical in advancing endoscopic surgical procedures, with the introduction of improved optics and lighting, advanced instrumentation, and image-guided surgical navigation. Hemostatic materials and devices have similarly evolved to assist in the management of the surgical field and the postoperative cavity.
Introduction
Functional endoscopic sinus and skull base surgery has become an effective part of the management of chronic rhinosinusitis and tumors of the sinuses and anterior skull base. Technologic advances have been critical in advancing endoscopic surgical procedures, with the introduction of improved optics and lighting, advanced instrumentation, and image-guided surgical navigation. Hemostatic materials and devices have similarly evolved to assist in the management of the surgical field and the postoperative cavity.
Discussion
- •
Decreased visualization can increase the risk of injury
- •
Early termination of surgery secondary to poor visualization
- •
Readmission or reoperation for the treatment of epistaxis
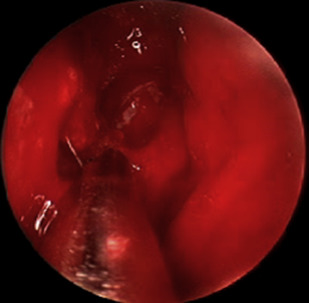
Hemostasis, both during and after endoscopic procedures, is critical for successful outcomes. Intraoperative bleeding, especially in the setting of highly vascular sinonasal tumors and polyposis, remains a common pitfall in performing endoscopic sinus and skull base surgery ( Fig. 1 ). Although endoscopic bipolar forceps; suction cautery; and newer technologies, such as radiofrequency coblation, are indispensable for producing intraoperative hemostasis, various topical agents are also effective in controlling diffuse bleeding and, in some cases, also provide postoperative benefits.
- •
Patient positioning
- •
Proper surgical technique
- •
Vasoconstriction
The primary modality to achieve hemostasis in surgery is the prevention of bleeding. The 3 steps to improve the ability to prevent bleeding are patient positioning, proper surgical technique with avoidance of stripped mucosa, and vasoconstriction. The patient’s head should be placed in the neutral anatomic position and the operative bed placed in 15° to 20° reverse Trendelenburg with total intravenous anesthesia. Proper surgical technique cannot be overemphasized to avoid nuisance bleeding. The stripping of mucosa causes oozing, which decreases visualization and is not amenable to topical vasoconstrictors. If persistent bleeding occurs in the absence of mucosal stripping, vasoconstrictors have an important role in endoscopic sinus and skull base surgery.
- •
Topical and injectable preparations
- •
Excellent hemostatic ability
- •
Potential for cardiac complications
Epinephrine has been used as a hemostatic agent in various surgical procedures for many years both in topical and injectable preparations. It is inexpensive and has excellent hemostatic properties. The major drawback to its use is the potential for cardiac complications, including tachycardia, arrhythmias, hypotension, or hypertension. Hypertension and tachycardia historically are the most commonly observed complications. Recently, use of topical epinephrine in endoscopic sinus and skull base surgery has experienced resurgence because topical preparations provide excellent hemostasis and greatly decrease the potential for cardiac complications.
The authors’ practice routinely uses epinephrine with Naropin (anesthetic benefit)-soaked cotton pledgets to aid with hemostasis. Our preferred concentration is 1:2000, which provides excellent hemostasis with limited side effects. A prospective study evaluating varying concentrations of topical adrenaline, including 1:2000, 1:10,000, and 1:50,000, showed that the 1:2000 group had a statistically significant decrease in blood loss and shorter operative times.
- •
Immediate problems include pain, rhinorrhea, infection, sensation of pressure, alar necrosis, and nasal obstruction
- •
Packing removal caries a risk of epistaxis
- •
Significant subjective decrease in surgical experience for the patient
Nasal packing with gauze was routinely used in the postoperative care of the nasal cavity but carries significant drawbacks. Packing can result in pain, rhinorrhea, infection, nasal obstruction, sensation of pressure, alar necrosis, and epistaxis on removal. Packing and the removal thereof has been reported as the most uncomfortable portion of the perioperative experience.
How have materials and devices in endoscopic sinus and skull base surgery evolved?
Nasal packing was historically the workhorse of hemostasis control in the postoperative cavity but caries significant risks. To move away from these inherent risks, topical materials that have absorbable properties or aid with hemostasis have become increasingly popular to help improve patient comfort, avoid the need for removal, and assist with healing. Although there are multiple products available ( Table 1 ), no single product provides a perfect solution to assist in postoperative care.
| Name | Composition | Hemostatic Ability | Scar Potential | Stent Ability |
|---|---|---|---|---|
| Tranexamic acid (Cyklokapron) | NA | Fair | Low | NA |
| Epsilon-aminocaproic acid (Amicar) | NA | Poor | Low | NA |
| FloSeal | Bovine gelatin + thrombin | Excellent | High | Fair |
| Surgiflo | Porcine gelatin | Good | Moderate | Fair |
| Sepragel | Cross-linked hyaluronic acid molecule | Fair | Low | Good |
| MeroGel | Hyaluronic acid ester | Fair | Low–high | Good |
| Seprapack | Hyaluron and carboxymethylcellulose | Fair | Low | Good |
| Microporous polysaccharide hemospheres (MPH) | Purified potato starch | Good | Low | Fair |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


