Fig. 34.1
Fundus phlebography: bilateral papilloedema with peripapillary haemorrhages ((a) right eye on admission, (b) right eye after treatment)
The re-evaluation of clinical history neither showed evidence of recent cranial/extracranial infection nor ongoing pharmacological treatment (oral contraceptives). There was no history of tick bites, joint pains or target rash. Her past medical, neurological, surgical, travel and family history was unremarkable. She had no known allergies. There was no evidence of neuroinflammatory or general immunological disorders in her family history. Her mother and her father were in good health, the patient being the first of three healthy sisters. She has a 10-year-old healthy child.
34.2 Differential Diagnosis and How to Work Up This Kind of a Patient
Considering the de novo headache with slowly increasing severity, with a partial and temporary response to the treatment and with subsequent onset of horizontal diplopia, a situation of increased intracranial pressure could be a first working hypothesis. In the presence of headache with increasing severity after weeks, followed by diplopia without other neurologic signs in a young, slightly overweight woman, the differential diagnosis versus other categories of secondary headache should be considered with a thorough workup.
Certain patients may face a sudden, somewhat severe, headache, hours/up to weeks preceding rupture of an intracranial aneurysm. This is generally referred as ‘sentinel headache’, which is usually short lasting, isolated or associated with general or focal neurologic symptoms/signs. In our case, considering a relatively long-lasting de novo headache, the search for an intracranial aneurysm is mandatory, headache symptoms being attributable to possible small bleeding from aneurysm and diplopia to direct compression of cranial oculomotor nerves. However, our patient did not have symptoms/signs of even minor meningeal irritation from SAH. However, inflammatory, infectious and neoplastic meningitis may eventually be present with isolated headache and diplopia (without other neurologic deficits and meningitis). But more frequently systemic symptoms and focal or general neurologic deficits (other cranial nerve palsies, cognitive/behavioural arousal dysfunction, etc.) became evident with time.
Once a dangerous secondary headache is excluded from aneurysm or other arterial malformations, other intravascular causes of persisting headache and diplopia should be considered, such as cerebral venous thrombosis, extracranial dissection and cranial arteritis. Most of these conditions should be ruled out by appropriate neuroimaging (standard plus neurovascular study) and lumbar puncture (neurosarcoidosis, neuroborreliosis, etc.).
Furthermore, local inflammatory causes should be ruled out such as orbital cellulitis/myositis and ENT complications, such as tumours or fungal infections of the anterior skull base.
On the other hand, the cause of severe persisting headache, possibly complicated by diplopia, dizziness and other minor symptoms, may be consistent with the diagnosis of idiopathic intracranial hypotension (IIH). This condition strictly is characterised by a typical orthostatic headache, being generated exclusively during the vertical position. Orthostatic headache in the presence of low CSF pressure (either spontaneous or secondary), or CSF leakage (spontaneous or secondary), is usually accompanied by neck pain, tinnitus, changes in hearing, photophobia and/or nausea. It remits after normalisation of CSF pressure or successful sealing of the CSF leakage (blood patch).
In our case, however, CSF pressure was increased (280 mm H2O).
Systemic disease as SLE, Behcet’s disease, uraemia, iron deficiency anaemia, Addison’s disease, hypothyroidism and polycystic ovarian disease might be associated with intracranial hypertension. The same goes for medications such as tetracycline, oral contraceptive pill, lithium, progesterone, growth hormone and steroid withdrawal.
Finally, ophthalmoplegic migraine has not included in the differential diagnosis, because it is not included in the ICHD-III beta version.
34.3 Topics for Analysis
34.3.1 How Do the Examinations Aid to Manage the Workup?
Bilateral optic disc swelling in the presence of normal optic nerve function is consistent with an increased intracranial pressure. Diagnosis of IIH is focused on symptoms only attributable to intracranial hypertension, ruling out vascular lesions, mass, or ventriculomegaly on neuroimaging, and other aetiology of intracranial hypertension established (Fig. 34.1).
Still, further causes of intracranial hypertension should be taken into account: inflammatory, infectious and malignant disorders involving the meninges, brain tumour and a venous sinus thrombosis.
A markedly elevated blood pressure (malignant hypertension) can also give rise to disc swelling in addition to headache, with a clinical picture different from the present case.
Any de novo continuous headache should be investigated with neuroimaging focusing on parenchymas, arterial/venous circulation and meninges.
In patients with evidence of papilloedema, neuroimaging should be performed prior to lumbar puncture, to exclude the risk of herniation and to search for any secondary cause of intracranial hypertension. CT or MR venography is requested to exclude cerebral venous sinus thrombosis.
If the neuroimaging does not show a mass lesion, obstructive hydrocephalus, or evidence of cerebral venous thrombosis, a lumbar puncture should follow to confirm the diagnosis of suspected ‘benign’ intracranial hypertension and to rule out malignant, infectious or inflammatory disorders simulating IIH symptoms and sign (Fig. 34.2).
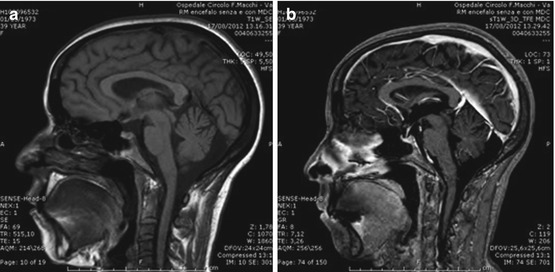
Fig. 34.2
(a) Basal brain MRI; (b) venous angio-MRI with gadolinium
The CSF examination should include cytology, bacteriology, full viral test (PCR and viral and syphilis markers) and serology for parasites and fungi. In some patients, especially children, an opening pressure of up to 280 mm CSF is normal, but, for most of the cases, an opening pressure above 280 mm CSF should be considered elevated.
Patients should also undergo blood tests including complete blood counts, erythrocyte sedimentation rate, coagulation, and electrolytes and tests for syphilis, thyroid function tests and electrophoresis.
In our patient, blood tests included complete blood counts, routine chemistry, erythrocyte sedimentation rate, C-reactive protein, coagulation panel, thyroid function tests, rheumatoid factor, antinuclear antibody, anti-ds-DNA antibody and antineutrophil cytoplasmic antibodies, which were all normal with the exception of positive ANA Ab (homogenous pattern 1:640).
Lumbar puncture showed a slightly elevated opening pressure (i.e. > 250 mm H2O) with normal laboratory profile (no white blood cell, 19 mg/dL of protein, 85 mg/dL of glucose, absence of oligoclonal banding).
34.4 Topics for Discussion
34.4.1 Which Is the Diagnosis? Which Is the Treatment for Our Patient?
Given the specific symptoms of headache and diplopia in a young slightly overweight female, associated with raised CSF pressure with normal CSF profiles, papilloedema and normal neuroimaging without other causes of intracranial hypertension, a diagnosis of IIH can be given.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


