Fig. 32.1
CT scan done on the third day of sudden-onset severe headache which shows hemorrhage within the anterior interhemispheric fissure and bilateral sylvian cisterns more prominent on the left
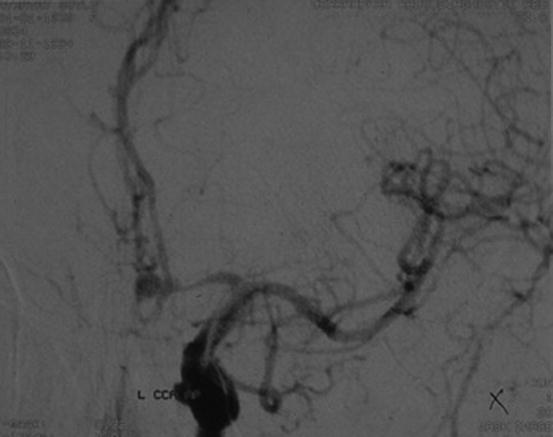
Fig. 32.2
Digital subtraction arteriography showing the left anterior communicating artery aneurysm and secondary arterial vasospasm
The patient was then referred to the department of neurosurgery, and two of the aneurysms, the one that bled at the left anterior communicating artery and the unruptured one at the bifurcation of the left middle cerebral artery, are clipped. She makes a complete recovery, and after a few weeks, she undergoes an endovascular closure of the aneurysm at the tip of the basilar artery with coiling.
32.4 Summary of the Case
A 55-year-old housewife with a sudden onset of “the worst headache of her life” is admitted to the ER after 3 days of the onset of her severe headache as it was not improving. She was first seen in another hospital soon after the onset but was told that her examination was normal and then was referred for a cranial CT scan. However, instead of having an emergency scan, she was given a late appointment. As she was not getting better then, she was readmitted to our ER. Her neurological and physical exams were insignificant, and there was no neck stiffness. Based on the features of her headache history which was consistent with an abrupt-onset head pain that reached its peak intensity within seconds to minutes and was accompanied with nausea and vomiting raised the suspicion of SAH or other diagnostic probabilities of either primary or secondary thunderclap headache types. Therefore, she was referred for an emergency CT scan which disclosed SAH. Following a DSA study that confirmed a ruptured aneurysm, as well as two others, she was treated first by surgery and later by an endovascular coiling procedure of which she made an uneventful recovery.
32.5 Definition of Subarachnoid Hemorrhage
According to “The International Classification of Headache Disorders, 3rd edition (beta version)” [Cephalalgia 2013; 33(9) 629–808], the definition of “headache attributed to nontraumatic subarachnoid hemorrhage (SAH)” is described as typically severe and sudden, peaking in seconds (thunderclap headache) or minutes.
This headache may be the sole symptom of SAH, and the diagnostic criteria will include the absence of head trauma supported with the demonstration that the development of headache was in close temporal relation to other symptoms and clinical signs of SAH and then improved in parallel with stabilization or improvement of other symptoms or clinical or paraclinical signs of SAH.
As expected with all other set of criteria, this headache should not be better explained by any other ICHD-3 diagnosis.
32.6 Brief General Information
SAH is a diagnosis which should not be missed as the mortality rate can be as high as 50 %. Depending on the severity of the bleeding, 10–20 % of patients may die before arriving at the hospital. Besides, a significant number of patients with SAH are left disabled. There is a risk of rebleeding which is 3–4 % during the first 24 h, about 1 % per day during the first month, and 3 % per year long-term risk after 3 months in unrepaired aneurysms. Other risks in a patient with SAH are vasospasm with delayed cerebral ischemia, hydrocephalus, elevated intracranial pressure, seizures, and hyponatremia. Approximately 85 % of SAHs are secondary to a ruptured intracranial saccular aneurysm, 10 % are caused by the benign perimesencephalic syndrome, and the remainder are caused by arteriovenous anomalies and other rare conditions. Most SAH headaches last days to weeks and initially nausea and vomiting occurs as well. Photophobia is also common. The probability of SAH is very low if the intensity of the severe headache develops over minutes to hours and the pain lasts less than one hour. The presence of any neurologic sign or impairment of consciousness increases the likelihood of an SAH or other underlying serious conditions.
The noncontrast-enhanced CT scan has a sensitivity of 98 % in the first 12 h after onset of the SAH, which drops to 93 % at 24 h and 50 % at 7 days. A CSF study will reveal xanthochromia in almost all cases with aneurysmal SAH when it is done within the first 12 h and 2 weeks after the onset of the symptoms and analyzed by spectrophotometry, but it should be kept in mind that in some patients, when the lumbar puncture (LP) is done very early, the bleeding may be missed. Recently, a CT-angiography (CTA) following a CT scan has been suggested as an alternative diagnostic strategy instead of performing an LP. However, there are also some concerns with this strategy, such as risks of additional radiation exposure (especially in the young!), time, and costs and comparability between LP and CTA. Besides, one of the other concerns is how to manage when incidental and asymptomatic aneurysms are discovered.
Key Points for Patients Who Are Admitted with “Sudden-Onset Very Severe Headaches”
Limited clinical data suggest that headaches requiring more than several minutes to peak in intensity are low risk for SAH.
However, although that abrupt onset of headache is always of concern for SAH, one study showed that this occurred only half of the time in patients with SAH.
Sudden-onset HA is seen more often in patients with benign causes of thunderclap headaches.
Nearly half of patients with SAH have headaches that deviate from the “classical” description.
No characteristic location has been determined; neck pain is common, but neck pain is also common in migraine.
In a large series of SAH, 34 % of headaches occurred during nonstrenuous activity and 12 % developed during sleep.
A past history of recurrent headaches, including their frequency and site and whether they were migrainous or not, was found not to be associated with the risk of SAH.
Key Points Regarding How to Work Up Patients Who Are Admitted with “Sudden-Onset Very Severe Headaches” and Suspected to Have Subarachnoid Hemorrhage
A sudden-onset “first or worst” nontraumatic headache, which reaches its maximal intensity within seconds to a few minutes and which lasts at least more than one hour, whether associated with any neurologic sign or not, should raise the probability of subarachnoid hemorrhage or other underlying life-threatening neurologic diseases.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


