7 Head and Neck Surgical Oncology
Tumor Biology and Carcinogenesis
1 | What are the five basic phases of the cell cycle, and what occurs during each phase? | • Quiescent phase (G0): Resting state • Gap 1 (G1): Preparation for cell division; increase in transcription/translation and ~ doubling of macromolecules • Synthesis phase (S): Replication of chromosomes • Gap 2 (G2): Continued cellular growth • Mitosis phase (M): Chromosomes are separated, and two daughter cells result |
2 | What is the term given to cells in permanent cell-cycle arrest? | Senescent |
3 | What are the key checkpoints within the cell cycle? | • G1/S checkpoint (“restriction point”): Prevent entry into S-phase, rate-limiting step • Intra-S phase checkpoint: Halt progression of S-phase if damaged DNA is detected • G2/M checkpoint: Prevent entry into M phase • M checkpoint: Ensure correct replication of DNA and avoid mitotic exit if errors exist |
4 | If a lesion (i.e., partially replicated DNA, strand breaks, or other errors) is identified at a checkpoint, what processes can be activated? | • Recruitment of DNA repair effector complexes • Temporary cell-cycle arrest, which can lead to senescence or apoptosis, depending on the cell and the lesion |
5 | What key tumor suppressor protein controls progression through the G1/S checkpoint (restriction point) and the G2/M checkpoint? | p53 (activates p21 → inhibits cyclin and cyclin-dependent kinase (Cdk) complexes) |
6 | What two key classes of molecules regulate a cell’s progress through the cell cycle? | • Cdk s: Catalytic subunit; require cyclin for activation; result in phosphorylation (activates/inactivates molecules necessary for progression through the cell cycle) • Cyclins: Regulatory subunit that activates Cdk molecules when bound to form a heterodimer |
7 | Although more than 15 Cdks have been identified, four have key biologic functions within the cell cycle. What are they, and what do they do? | • Cdk 1: Controls G2 phase and M phase (prophase) → Cyclin A dependent • Cdk 2: Controls G1 to S transition and S phase → cyclin E (and A) dependent • Cdk 4: G0 to G1 transition → cyclin D dependent • Cdk 6: G0 to G1 transition → cyclin D dependent |
8 | Specific families of activators and inhibitors regulate functional activities of the Cdk complexes. Identify the primary activators and inhibitors. | • Activators: Cdk-activating kinase (CAK) and Cdc-25 • Inhibitors: Cdk inhibitors (CKI) → Inhibitor of kinase 4 (INK4a), Cdk Interacting protein/kinase inhibitory protein (Cip/Kip) |
9 | What type of gene helps to control cell growth or progression through the cell cycle? | Tumor suppressor gene (also called antioncogenes) |
10 | What type of gene promotes cell growth and progression through the cell cycle? | Proto-oncogenes. Once a proto-oncogene is mutated, it is known as an oncogene. |
11 | The classic retinoblastoma tumor suppressor protein (pRb) functions to inhibit what key transcription factors, effectively preventing formation of cell cycle–related proteins and arresting the cell in G0 phase? | E2F factors |
Phosphorylation of pRb by what important cyclinCdk complex (es) results in dissociation of pRb from E2F and subsequent entrance into the cell cycle? | Cyclin D-Cdk4 and cyclin D-Cdk6 | |
13 | Release of E2F from pRb inhibition results in the transcription of multiple genes necessary for the function of the cell cycle. Transcription of what key cyclin protein results in activation of Cdk2, progression from G1 to S phase, additional pRb inactivation, and p27 degradation? | Cyclin E |
14 | What genes are considered members of the Cip/Kip family of tumor suppressor genes, and in what phase of the cell cycle do they inhibit cyclin-Cdk complexes? | • p21, p27, and p57 • G1 phase |
15 | DNA damage results in activation of what key tumor-suppressor gene and proapoptotic factor, which in turn activates p21 (a Cip/Kip Cdk complex inhibitor) and results in arrest of the cell cycle in G1 phase? | p53 |
16 | Transforming growth factor-β is a growth inhibitor, which results in activation of which INK4 tumor suppressor gene causing subsequent cell-cycle arrest in G1 phase? | p27 |
17 | What genes are considered members of the INK4a family of tumor-suppressor genes, and in what phase of the cell cycle do they inhibit cyclin-Cdk complexes? | • p16 and p19 • G1 phase |
18 | Name the tumor suppressor gene that is a member of the INK4a family that prevents p53 degradation and therefore results in cell-cycle arrest at the G1-checkpoint. | p19 |
19 | Name the tumor suppressor gene that is a member of the INK4a family that inhibits cyclin DCdk4/6 complexes and therefore results cell cycle arrest during the G1 phase. | p16 |
20 | What important enzymes function to dephosphorylate the targets of cyclin-Cdk complexes, such as pRb? | PP1 and PP2A (phosphatases) |
21 | To promote an orderly progression through the cell cycle, cyclin-Cdk complexes must be degraded to allow the next phase of the cell cycle to progress uninterrupted. For example, S-phase complexes cannot be active during M phase and so forth. What important enzymatic process selectively targets these complexes for degradation? | Ubiquitin-dependent protein degradation (ubiquitylation) |
22 | The phases G1, S, and G2 are collectively referred to as what? | Interphase |
23 | What are the five stages of mitosis (M phase)? | • Prophase: Preparatory; cyclin A-Cdk1 active; condensation of chromatin, polarization of centrosomes, and initiation of mitotic spindle formation • Prometaphase: Nuclear envelope breaks down, mitotic spindle microtubules attach to chromosomes • Metaphase: Alignment of chromosomes at metaphase plate • Anaphase: Separation of sister chromatids • Telophase: Cytoplasmic division (cytokinesis) into two daughter cells; chromatid decondensation (expansion) |
Describe the “two-hit” hypothesis (Knudson, 1971) for carcinogenesis. | Loss of two alleles for a tumor-suppressor gene is necessary to result in loss of function and tumorigenesis. This hypothesis is not applicable to proto-oncogenes and dominant negative tumor suppressor genes (e.g., p53). | |
25 | In an effort to understand carcinogenesis, Fearon and Vogelstein (Cell, 1990) presented a model of tumor progression that involved which three hypotheses? | • Inactivation of tumor suppressor genes or activation of proto-oncogenes results in the formation of cancer. • A series of defined genetic events lead to the development of cancer. • This linear progression may vary, but ultimately it is the accumulation of genetic events that results in the development of a malignant phenotype. |
26 | What is the estimated average of time required for the accumulation of enough genetic alterations to produce traditional head and neck squamous cell carcinoma (Renan, 1993)? | 20 to 25 years |
27 | Carcinogenesis models describe a linear progression from precancerous lesions to overtly malignant tumors. Describe the steps involved for each of the following models: 1. Genetic progression model for head and neck cancer 2. Multistep carcinogenesis | 1. Hyperplasia → dysplasia (mild, moderate, severe) → carcinoma in situ → invasive carcinoma 2. Initiation → promotion → progression |
28 | In upper aerodigestive tract tumors, what term describes the histopathologic changes seen in mucosa surrounding invasive carcinoma and result in an increased incidence of second primary tumors? | Field cancerization (Slaughter, 1953) |
29 | What hypotheses focusing on the clonal abnormality required for tumor growth have been put forth to explain field cancerization? | • Abnormal, and genetically unique, clones form independently at multiple sites due to exposure to similar environmental carcinogens. • A single tumoral clone forms and subsequently migrates via lateral movement through the mucosa (shown in several studies to be accurate). |
30 | What are the two predominant environmental carcinogens that have been associated with head and neck cancer, show a dose response, and can function synergistically? | • Tobacco • Alcohol |
31 | Why might alcohol, in particular, function as a synergistic carcinogen with other environmental carcinogens? | It may decrease the effectiveness of both local and systemic detoxification enzymes (e.g., cytochrome P450 system). |
32 | Does cessation of smoking and alcohol consumption reduce the risk of head and neck cancer development? If so, how long does it take for the risk to reach the level of never-smokers? | Yes. Some studies have shown 20 years or longer. |
33 | How does diet impact the development of cancer of the upper aerodigestive tract? | A high intake of fruits and vegetables and low intake of red meat or processed meats has been associated with a decreased risk of head and neck cancer (INHANCE Consortium, 2012). |
34 | Describe the cell-cycle dysregulation that is commonly seen in patients with environmentally related head and neck cancer. | (Posner, Goldman’s Cecil Medicine, 24th ed., Chp196) • Loss of p16 (normally inhibits cyclin D) • Upregulation of cyclin D • Loss of p53 (normally inhibits cell cycle progression and promotes apoptosis) • Upregulation of EGFR (enhances mitogenic signaling) • Upregulation of COX-2 (increased angiogenesis, decreased apoptosis) • Increased chromosomal instability (increased aneuploidy) |
What genetic conditions are related to an increased risk of head and neck cancer? | • Fanconi anemia (AR; DNA repair gene mutation) • Cowden syndrome (AD: PTEN hematoma tumor syndrome; PTEN is a tumor suppressor gene) • Mutations in the cytochrome P450 enzymes (CYP1A1 mutations in Asian populations) | |
36 | What circular, double-stranded DNA virus commonly infects the basal layer of cutaneous of mucosal squamous epithelium and is spread by sexual contact? | Human papilloma virus (HPV) |
37 | What two HPV strains are considered “low-risk” for the development of cancer and are frequently associated with papillomas and warts? | HPV 6 and 11 |
38 | What two HPV strains are considered “high-risk” for the development of cancer and have been associated with cervical, anogenital, and head and neck (predominantly oropharyngeal) carcinomas? | HPV 16* and 18 *90% of HPV (+) head and neck carcinomas |
39 | The HPV DNA encodes nine open reading frames (genes) on a single strand of its double-stranded circular DNA. Seven of these are considered early phase genes (E), and two are considered late-phase genes (L). What are the general functions of the E and L genes, respectively? | • E genes: Regulate the transcription viral DNA • L genes: Encode capsid proteins involved in viral spread |
40 | Name the two viral onco-proteins in HPV-related tumorigenesis, and identify the two genes, that control the transcription of these viral proteins. | • E6/E7: Onco-genes • E1/E2: Transcriptional regulators |
41 | When HPV DNA integrates into host DNA, the process can result in deletion or loss of function of the E1 and E2 viral genes. This in turn results in what? | Loss of regulation of E6 and E7and subsequent increased transcription of these viral genes |
42 | What HPV protein functions to inhibit the function of p53 by targeting it for ubiquitin-dependent degradation? What is the result? | • E6 • Progression through G1 checkpoint and inhibition of apoptosis |
43 | What HPV protein phosphorylates pRb and thus targets it for ubiquitin-dependent degradation? What is the primary result? | • E7 • Release of pRb inhibition of E2F, activation of cell cycle-related transcription, progression through the G1 checkpoint |
44 | In addition to E2F-related transcription, the degradation of p53 results in over expression of what important protein? What impact does this have on cell-cycle progression? | • p16 • Normally inhibits Cdk4/6, but with the los of p53 and pRb, does not meaningfully result in cell cycle control. Can be used as a biomarker of HPV activity. |
45 | In addition to HPV, what viruses have been associated with head and neck cancer? | • Epstein-barr virus (EBV): Nasopharyngeal carcinoma • Human immunodeficiency virus (HIV): Increased risk of head and neck cancers • Merkel cell polyomavirus: Merkel cell carcinoma • Human T-lymphotrophic virus (HTLV-1): Human T-Cell lymphoma/leukemia • Kaposi sarcoma associated herpesvirus (KSHV): Kaposi sarcoma |
46 | Whereas the epidermal growth factor receptor (EGFR) is normally expressed in the epithelium of several organ systems (dermis, gastrointestinal tract, kidney), it has been found to be dysfunctional in what percentage of head and neck (squamous cell) cancers? | 80 to 90% |
EGFR is a transmembrane glycoprotein that, when activated by binding an extracellular ligand, results in dimerization, tyrosine kinase activation, and a complex downstream pathway that ultimately results in what major outcomes? | • Cellular growth and proliferation • Apoptosis • Angiogenesis • Invasion • Metastasis | |
48 | How does EGFR expression relate to prognosis in head and neck squamous cell carcinoma? | Increased expression and amplification are related to decreased recurrence-free survival and cancer-specific survival rates. |
49 | What strategies have been used to target aberrant signaling in head and neck squamous cell carcinoma based on a better understanding of EGFR signaling? | • Tyrosine kinase inhibitors (geftinib) • Monoclonal antibodies inhibiting dimerization (cetuximab) • Antisense oligodeoxynucleotide or small interfering mRNA inhibition of mRNA expression |
50 | What immune cell is primarily responsible for identifying normal cells that have been altered by viral or tumor activity? What is the general function of these cells in patients with head and neck cancer? | T cells Decreased: T cells demonstrate increased apoptosis, decreased recruitment from the thymus, and poor proliferation. Overall immunosuppression |
51 | What important normal immune system function is designed to prevent the recognition of “self” through processes such as anergy, suppression, and ignorance, which makes stimulating the immune system to target self-derived tumor cells challenging? | Tolerance |
52 | What cell-based therapeutic model has been studied in head and neck cancer with promising (although early) results that focuses on using the immune system to target cancer cells specifically? | Immunotherapy focused on manipulation of the following: • Cell signaling (i.e., cytokines such as interleukin-2) • Vaccination (i.e., Gardasil, whole-cell vaccines, dendriticcell vaccines, etc.) • T cells, dendritic cells, or antibodies |
53 | What type of therapy has the potential to prevent head and neck cancer from occurring, recurring, or progressing? | Chemoprevention |
54 | What prominent chemopreventive agents have been studied for use in patients with head and neck cancer? | • Retinoids and vitamin A (betacarotene) • COX-2 inhibitors • Aspirin • Selenium • Vitamin D • Interpheron-α2a • α-tocopherol (Vitamin E) Many others are being studied. There is great controversy surrounding most of these agents as studies have demonstrated conflicting results. |
55 | What chemopreventive effects are retinoids purported to have on head and neck cancer? | They can retard progression of premalignant oral lesions (leukoplakia and erythroplakia) and have also been associated with lower rates of second primary tumors. Subsequent studies have called these results into question. |
56 | True or False. The risk of head and neck cancer increases in the setting of vitamin A toxicity. | False. The risk increases with vitamin A deficiency. |
57 | What inflammatory mediator is elevated in head and neck cancer cells? | Prostaglandins as a result of the upregulation of COX-1 and -2 |
Principles of Staging Evaluation and Prognosis
58 | What oncologic staging system was devised in 1959 by the American Joint Committee on Cancer (AJCC) to describe the extent of the primary tumor, involvement of regional lymph nodes, and metastases to distant sites in an effort to form a cohesive system providing the clinician with an important tool to predict prognosis, counsel the patient, chose an intervention, and perform more consistent clinical research? | Tumor, node, metastasis (TNM) staging system |
Using the TNM staging system, how can you differentiate a clinical stage from a pathologic stage? | • Clinical stage is designated with a “c” and is based on physical examination or imaging (e.g., cT, cN, or cM). • Pathologic stage is designated with a “p” and is based on pathologic analysis of a specimen (e.g., pT, pN, pM). | |
60 | Which subsites share the following criteria (in addition to subsite specific criteria) for T staging: • T1: < 2 cm • T2: > 2 cm, < 4 cmT3: > 4 cm | • Lips and oral cavity • Oropharynx • Hypopharynx (plus additional criteria) • Major salivary gland (plus additional criteria) • Well-differentiated thyroid cancer and medullary thyroid cancer (plus additional division of T1a, T1b) |
61 | In the 7th edition of the AJCC, the terms resectable and unresectable were changed to mean “moderately advanced local disease (T4a)” and “very advanced local disease (T4b)” in an effort to predict better the prognosis using current management strategies. What does “very advanced local disease” generally represent? | Very advanced disease correlates with extension into surrounding critical structures which are largely viewed as unresectable or incurable. |
62 | The following head and neck subsites share what nodal (N) staging system? • Oral cavity • Oropharynx • Hypopharynx • Larynx • Nasal cavity and paranasal sinuses • Major salivary glands | ( |
Table 7.1 AJCC neck (N) staging for head and neck tumors (excluding nasopharynx and thyroid).
Stage | Description |
NX | Cannot assess |
N0 | No regional metastasis |
N1 | Single ipsilateral lymph node, ≤ 3 cm |
N2a | Single ipsilateral lymph node, > 3 cm but ≤ 6 cm |
N2b | Multiple ipsilateral lymph nodes, ≤ 6 cm |
N2c | Bilateral or contralateral lymph nodes, ≤ 6 cm |
N3 | Lymph node > 6 cm |
Data from Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, eds. AJCC Cancer Staging Manual 7th Edition. New York, NY: Springer; 2010. | |
63 | What two head and neck subsites have a unique nodal staging system compared with the majority of subsites? | • Nasopharynx • Thyroid |
64 | Using the TNM staging system, the lips, oral cavity, oropharynx, hypopharynx, larynx, nasal cavity, paranasal sinuses, and salivary glands can all be staged based on what system? | ( |
Table 7.2 TNM staging system for most head and neck cancers (lips, oral cavity, oropharynx, hypopharynx, larynx, nasal cavity, paranasal sinuses, and salivary glands).
Stage | TNM description |
I | T1 N0M0 |
II | T2 N0M0 |
III | T3N0M0, T1–3N1 M0 |
IVA | T4aN0–2M0, T1–3N2 M |
IVB | T4b AnyNM0, AnyTN3 M |
IVC | AnyTAnyNM1 |
Data from Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, eds. AJCC Cancer Staging Manual 7th Edition. New York, NY: Springer; 2010. | |
65 | Tumor invasion of what subsites are considered by some as unresectable? | • Nasopharynx • Prevertebral fascia • Base of skull • Intracranial extension • Mediastinum • Subdermal lymphatics • Carotid artery encasement (generally > 270 degrees) |
66 | Describe how the American Joint Committee on Cancer reports the presence or absence of residual tumor (R) following treatment. | • RX: Residual tumor cannot be assessed • R0: No residual tumor • R1: Microscopic residual tumor • R2: Macroscopic residual tumor |
67 | How does the AJCC recommend reporting tumor grade? | • GX: Grade cannot be assessed • G1: Well differentiated • G2: Moderately differentiated • G3: Poorly differentiated • G4: Undifferentiated |
68 | Patients with head and neck cancer will have symptoms related to the location and extent of their tumor that are often subsite specific. What “red flag” signs or symptoms should be reviewed with all patients who have concerns for head and neck cancer? | Pain, cranial neuropathy, bleeding, unintentional weight loss, lymphadenopathy, malaise, anorexia |
69 | What risk factors should be elicited when taking a history on a patient with potential head and neck cancer? | • Tobacco* (smoked and smokeless) and alcohol* exposure • Viral infection (EBV and HPV*) • Radiation exposure • Diet low in fruits and vegetables and high in red meats and processed meats • Occupational risk factors such as woodworking, textile exposure, and nickel refining • Sun exposure • Personal history of head and neck cancer • Family history of cancer • Poor dentition, chronic inflammation, or chronic irritation • Immunosuppression • Use of betel (quid or panna) (Asia) * Major risk factors in developed countries |
70 | What risk factors are associated with advanced head and neck cancer at presentation? | • Low income • Black race • Poorly differentiated tumors • Patient neglect |
Define the Eastern Cooperative Oncology Group (ECOG) performance status system. | • Grade 0: Fully active, able to carry on all predisease performance without restriction • Grade 1: Restricted in physically strenuous activity but ambulatory and able to carry out work of a light or sedentary nature • Grade 2: Ambulatory and capable of all self-care but unable to carry out any work activities. Up and about > 50% of waking hours • Grade 3: Capable of only limited self-care; confined to bed more than 50% of waking hours. • Grade 4: Completely disabled; cannot carry out any self-care. Totally confined to bed or chair. • Grade 5: Deceased | |
72 | During a head and neck examination in an adult patient, you note unilateral serous otitis media. On flexible endoscopic examination, to what anatomical region(s) should you pay particular attention? | Posterior nasal cavity, nasopharynx, fossa of Rosenmuller and eustachian tube orifice |
73 | During fiberoptic or mirror laryngoscopy, what maneuvers are critical for a complete oncologic head and neck examination? | • Phonation → assess vocal cord mobility • Tongue protrusion → full view of the epiglottis and vallecula • Puff out cheeks → full view of pyriform sinuses and postcricoid region |
74 | You perform an otoscopic examination on a patient complaining of otalgia but note no obvious source of pain. Which nerve(s) might be implicated in referred otalgia? | CN V3, IX (via Jacobson nerve), X (via Arnold nerve), and VII (via the Ramsay Hunt branch of VII), as well as branches from C2 and C3 through the great auricular nerve |
75 | On evaluation of a primary head and neck tumor, in addition to the location and size of the tumor, what information can be gained from palpation that is critical to the workup? | Fixation of the tumor Note: fixation of nodal metastases should also be noted. |
76 | What premalignant lesion can present as a thickened white patch that can’t be scraped off on physical exam of the upper aerodigestive tract mucosa that can progress to invasive carcinoma in up to 30% of patients over a variable number of years? | Leukoplakia |
77 | What premalignant mucosal lesion can appear as a flat red patch with a malignant potential of up to 60% over a variable number of years? | Erythroplakia |
78 | What common initial screening test evaluates for pulmonary disease (metastases or primary lung cancer)? | Chest radiograph. PET/CT is also often ordered now as the initial screening test for distant metastases. |
79 | Which imaging modality is used most often in the initial workup of head and neck cancer patients? | Contrast-enhanced CT |
80 | CT scan of the head and neck is often ordered as a first-line imaging modality to evaluate the size, extent, and location of the primary tumor; status of the vasculature; and nodal disease. Should this scan be ordered with or without contrast? | With contrast (as patient’s allergies and renal status permits). In the initial workup of differentiated thyroid carcinoma, avoidance of iodinated contrast should be considered. |
81 | What are frequently used as radiographic criteria for a nodal malignancy on CT scan? | • Size > 1 cm • Evidence of central necrosis (~100% specificity) • Spherical shape (suggestive) • Nodal grouping in the predicted drainage pathway, with nodes > 1 cm |
What is a key disadvantage of CT scans when evaluating an oral cavity or oropharyngeal neoplasm in a patient with tooth fillings? | Dental artifact often obscures anatomy/pathology. | |
83 | In what situations is evaluation with MRI most useful during the workup for head and neck cancer? | • Soft tissue tumor (e.g., base of tongue, infratemporal fossa, parapharyngeal space, parotid) • Intracranial extension or skull base involvement • Paranasal sinus disease (e.g., inspissated secretions vs. tumor) • Nasopharyngeal tumors • Temporal bone • Assessment of perineural invasion |
84 | When is a PET/CT scan indicated during the treatment of a patient with head and neck cancer? | • Evaluation of equivocal disease • Workup of an unknown primary tumor (can identify up to a third of primary tumors) • Evaluate nodal disease (studies argue against its use in the cN0 neck) • Evaluate for distant metastases (may see a high number of false-positives but has a very high negative predictive value) • Surveillance after treatment |
85 | True or False. All head and neck tumors are PET avid because of their high metabolic activity. | False. Several head and neck tumors have either variable/inconsistent or no FDG-avidity. These include • Well-differentiated thyroid cancer • Medullary thyroid cancer • Indolent lymphomas • Neuroendocrine tumors • Teratomas • Soft tissue sarcomas |
86 | Why is it difficult to use a PET/CT scan to determine the extent of a skull base tumor? | Brain metabolism is high, which can obscure skull-base tumors, or tumors with intracranial invasion. |
87 | What might result in a false-positive result on a PET/CT scan? | • Infection • Normal physiologic activity • Inflammation (e.g., after radiation, surgical resection or biopsy, aspiration) • Osteoradnionecrosis • Granulomatous disease • Patient movement |
88 | What is one of the major limitations of PET/CT scanning, which can result in a false-negative scan? | It is unreliable for lesions < 1 cm in diameter (some scanners can reportedly detect suspicious lymph nodes as small as 5 mm). |
89 | What is the sensitivity of PET scan for detecting squamous cell carcinoma recurrence less than 1 month after completion of radiation therapy? More than 1 month afterward? | 55%, 95% Key issue: Waiting 3 months after completion of radiation minimizes false-positives resulting from inflammation and continued tumor regression. Patients should be clinically assessed for tumor progression during or after therapy, and patients with progression or bulky (N3) disease may require restaging and salvage sooner. |
90 | In addition to a CT scan, what imaging modality can be helpful for preoperative planning in a patient with a tumor invading the mandible that will require mandibulectomy or in a patient undergoing radiation therapy? | Panorex |
91 | Although ultrasound is not often used for the workup of nodal or primary head and neck cancer (other than thyroid disease), it is often used to assist in what important diagnostic procedure? | FNA biopsy. CT-guided biopsy can also be considered. |
When should an excisional lymph node biopsy be considered? | It is not indicated for most head and neck cancers (e.g.,, squamous cell carcinoma). If there is concern for hematoproliferative malignancy, excisional biopsies are often necessary to provide adequate tissue for evaluation. | |
93 | Incisional biopsies are routinely performed in the office setting for accessible tumors, such as oral cavity or oropharyngeal, to obtain a tissue diagnosis. Some clinicians recommend delaying this until after what key step in the workup? | Imaging |
94 | What is the most common pathologic type of cancer in the head and neck (excluding salivary and thyroid tumors)? | Squamous cell carcinoma (> 90%) |
95 | Which immunohistochemical marker is most commonly associated with neural/cartilaginous tumors, melanoma, and Langerhans cell histiocytosis? | S-100 |
96 | Which immunohistochemical marker is associated with carcinomas and papillomas? | Cytokeratin |
97 | Which immunohistochemical marker(s) is/are associated with melanoma? | • S-100 • HMB-45 • Melanoma-associated antigen recognized by T cells (MART-1) (diagnostic) |
98 | Which immunohistochemical marker is associated with neuroendocrine tumors (e.g., Merkel cell carcinoma, paraganglioma)? | • Neuron-specific enolase (NSE) • Chromogranin • Synaptophysin |
99 | Which immunohistochemical marker is most commonly associated with lymphoma? | • Leukocyte common antigen (LCA/CD45) • CD-20 → B-cell specificity • CD-3 → T-cell specificity |
100 | Which tumors stain positive for vimentin on immunohistochemistry? For desmin? | • Vimentin → sarcomas, lipomas, myomas • Desmin → sarcomas, myomas |
101 | Describe the World Health Organization (WHO) classification of mild, moderate, and severe dysplasia. | ( |
Table 7.3 The World Health Organization (WHO) classification of dysplasia.
Grade | Description |
mild | nuclear atypia and architectural abnormalities of epithelial maturation confined to the basal third of the epithelium |
moderate | abnormalities extend to the middle third of the epithelium |
severe | abnormalities extend into the superficial third of the epithelium |
carcinoma in-situ | full-thickness abnormalities without invasion beyond the basement membrane |
102 | What subtypes of squamous cell carcinoma of the head and neck have distinct clinical behaviors? | • Basaloid • Verrucous (< 5%) • Spindle cell • Adenosquamous |
What subtype of squamous cell carcinoma is commonly seen in HPV-positive oropharyngeal tumors (tonsil and base of tongue) and are more likely to present at an advanced stage owing to early nodal and distant metastases? | Basaloid carcinoma. Note: Despite the early regional metastases, these tumors are fairly sensitive to treatment and therefore have a better prognosis than conventional squamous cell carcinoma. | |
104 | Describe the histopathology for spindle cell carcinoma. | Spindle cell carcinoma is also called carcinosarcoma or pseudosarcoma because it includes a squamous cell lesion on the surface and a more notable underlying malignant spindle cell component. Currently, it is thought that the tumor arises from epithelial cells and then undergoes mesenchymal differentiation. |
105 | Why are spindle cell carcinomas, which are a subtype of squamous cell carcinoma, most commonly found in the oral cavity and larynx, also known as sarcomatoid, carcinosarcoma, or pseudosarcoma? | • Contains a superficial squamous cell lesion and a deeper malignant spindle cell component. • Stain positive for both cytokeratin (epithelial cells) and vimentin (mesenchymal cells). • Arises from epithelial cells and then undergoes mesenchymal differentiation. |
106 | What is the management strategy of choice for spindle cell carcinomas? | The strategy is controversial because of the limited numbers of case reports in the literature. Most recommend surgery. There is controversy about the radiosensitivity of the tumor. |
107 | How can adenosquamous carcinoma be distinguished from mucoepidermoid carcinoma? | Mucoepidermoid carcinoma does not include a mucosal component. Adenosquamous carcinoma has a predominant mucosal squamous cell component and a deeper adenocarcinoma component. |
108 | What squamous cell carcinoma subtype manifests as a slow-growing, velvety, exophytic, and warty mass in elderly patients, and what pathologic feature determines their prognosis? | • Verrucous carcinoma • Focal areas of high-grade squamous cell carcinoma |
109 | What is the preferred management for localized verrucous carcinoma? | Complete surgical resection. Surgery was superior to primary radiation in 5-year survival (89 vs. 58%). |
110 | What are the most common sites of metastasis for head and neck squamous cell carcinoma? | • Lungs (66%) • Bone (22%) • Liver (10%) • Less often skin, mediastinum, and bone marrow |
111 | Traditionally, what single prognostic factor has been shown to decrease overall survival by as much as 50%? | Regional nodal disease (N +) |
112 | When considering nodal disease, what factors have been considered negative prognostic features? | • Presence of nodal disease (decreases survival by as much as 50%) • Increasing nodal size • Extracapsular spread • Bilateral neck disease • Matted lymph nodes • Disease in levels IV and V • “Skipped” levels • Invasion of local structures by nodal disease • Confluence of primary disease and nodal disease • Total number of involved lymph nodes |
113 | During the radiologic workup for a patient with head and neck cancer, in addition to the information needed to provide a TNM stage, what specific radiologic feature regarding the primary tumor size has been identified as negative prognosticator? | Gross tumor volume (poorer locoregional control and overall survival). Note: Standardized uptake values (SUVs) for PET/CT scans have been investigated but results are inconclusive. |
What tumor biomarkers can be used to help determine prognosis in head and neck cancer? | • EGFR amplification and overexpression • HPV status • Loss of heterozygosity (suggests a loss of tumor suppressor gene function) • Aneuploidy | |
115 | When considering head and neck cancer as a whole, what are the most important contributors to overall cancer specific mortality? | • Locoregional recurrence (50 to 60%) • Distant metastases (20 to 30%) • Second primary disease (10 to 20%) |
116 | What comorbidities most commonly impact the choice of therapeutic intervention in head and neck cancer patients (therapeutic comorbidity)? | • Severe lung disease and poor pulmonary function (e.g., not a candidate for a supraglottic laryngectomy) • Renal failure, hearing loss, neurologic disorder (e.g., choice of chemotherapeutic agents or therapy) • Severe atherosclerotic disease (e.g., may not be a candidate for free tissue transfer reconstruction) |
117 | What comorbidities have been found to negatively impact prognosis in head and neck cancer (prognostic comorbidity)? | • Recent myocardial infarction or ventricular arrhythmia • Severe hypertension • Severe hepatic disease • Recent severe stroke |
Overview of Oncologic Therapy
118 | What defines the ratio of therapy resulting in therapeutic effect to the amount that results in toxicity or mortality? | Therapeutic ratio or index |
119 | What type of treatment regimen uses only surgery or radiation therapy for curative intent? | Single-modality treatment. Any approach using more than one treatment modality is considered multimodality or combined modality. |
120 | What treatment approach uses chemotherapy and/or radiation therapy before definitive therapy? | Neoadjuvant/Induction therapy |
121 | What treatment approach uses chemotherapy and radiation therapy together as the primary treatment modality? | Concurrent (concomitant) therapy |
122 | What treatment approach uses radiation therapy with or without chemotherapy after primary surgical management? | Adjuvant therapy |
123 | What treatment approach uses surgery, chemotherapy, and/or radiation for patients with recurrent or metastatic disease without the intent to cure? With the intent to cure? | • Palliative therapy • Salvage therapy |
124 | Define the three types of clinical trials. | • Phase I: Defines the maximum tolerated dose or safety of a drug or invasive medical device • Phase II: Includes more patients than phase I; assesses the efficacy and side effects or toxicity associated with the intervention of interest • Phase III: Randomized prospective trial comparing the intervention of interest with the standard of care; at termination, can be considered for Food and Drug Administration approval for the intervention of interest. |
125 | What tumors are considered by the National Comprehensive Cancer Network (NCCN, 2011) to be very advanced and therefore managed with a unique algorithm regardless of tumor subsite? | T4b, any N, M0 or unresectable nodal disease |
The NCCN (2011) recommends either a clinical trial or standard therapy for patients diagnosed with very advanced head and neck cancer. How is standard therapy individualized, and what does it include? | ECOG performance status (PS): • PS 0–1: Concurrent chemoradiation therapy with cisplatin or induction chemotherapy followed by radiation or chemoradiation therapy • PS 2: Definitive radiation therapy or concurrent chemoradiation therapy • PS 3: Radiation therapy vs. single-agent chemotherapy vs. best supportive care Note: With improvement in surgical management reconstructive techniques, some authorities suggest that surgical management should be considered for some T4b tumors. | |
127 | Patients with recurrent or persistent head and neck cancer after primary management are considered by the NCCN (2011) to have very advanced head and neck cancer. For patients who do not have distant metastases, what are the treatment options? | • Locoregional recurrence without prior radiation therapy
• Locoregional recurrence or second primary with a history of prior radiation therapy
|
128 | What is the standard therapy recommended by the NCCN (2011) for metastatic head and neck cancer? | Based on ECOG performance status (PS): • PS 0–1: Combination or single agent chemotherapy → best supportive care • PS 2: Single-agent chemotherapy or best supportive care → best supportive care • PS 3: Best supportive care |
129 | What percentage of patients with locally advanced head and neck squamous cell carcinoma die from recurrent locoregional disease within five years of initial treatment? | 30 to 50% |
130 | What is the median length of survival for a patient diagnosed with locally advanced or metastatic head and neck squamous cell carcinoma? | 6 to 9 months |
131 | What are the primary goals of palliative therapy? | • Improve quality of life • Prolong life |
132 | What prognostic factors predict poor outcome for patients with incurable head and neck squamous cell carcinoma? | • Poor performance status • Extensive tumor burden • Malnutrition • Prior history of extensive definitive therapeutic intervention • Rapid recurrence or progression |
133 | What is the general surveillance schedule for history of physical examination and imaging as recommended by the NCCN (2011) for head and neck cancer? | History and physical examination • Year 1: Every 1 to 3 months • Year 2: Every 2 to 4 months • Year 3 to 5: Every 4 to 6 months • > 5 years: Every 6 to 12 months Imaging • Within 6 months of treatment end for T3–4 or N2–3 cancers of the oropharynx, hypopharynx, glottic larynx, supraglottic larynx, and nasopharynx • Additional imaging based on concerning signs and symptoms |
134 | When should you evaluate a patient’s thyroid-stimulating hormone (TSH) level after completion of treatment for head and neck cancer? | If the neck was irradiated, check a TSH every 6 to 12 months. |
What are the three functional outcomes that are most commonly assessed for head and neck cancer? | • Airway • Speech • Swallowing | |
136 | What focuses on a patient’s perception of the impact of illness before, during, and after treatment? | Health-related quality of life |
137 | What domains are generally included in health related quality of life? | • Physical/somatic • Functional • Social • Psychological/emotional |
 Resectable: Surgery ± adjuvant therapy (for adverse risk features) vs. primary chemoradiation therapy
Resectable: Surgery ± adjuvant therapy (for adverse risk features) vs. primary chemoradiation therapy Unresectable: individualized based on performance status to nonsurgical treatment
Unresectable: individualized based on performance status to nonsurgical treatment Resectable: Surgery ± reirradiation ± chemotherapy
Resectable: Surgery ± reirradiation ± chemotherapy Unresectable: Reirradiation ± chemotherapy vs. palliative care
Unresectable: Reirradiation ± chemotherapy vs. palliative careOverview of Surgical Therapy
138 | What are the three major categories that should be considered when determining candidacy for surgical intervention for head and neck cancer patients? | • Physiologic: Cardiorespiratory fitness, coagulation status, immune status, and weight loss (> 10% body weight considered poor prognosticator for surgical intervention) • Anatomical: Surgical access to the subsite of interest (e.g., trismus in oropharyngeal cancer, brittle cervical spine or large osteophytes in laryngeal cancer) • Oncologic: Ability to achieve surgical margins, acceptable morbidity with complete resection |
139 | When considering surgical management of a primary head and neck tumor, what is a critical component of successful management? | Ability to achieve negative margins |
140 | For upper aerodigestive tract tumors, what is the minimum width of tissue that must be taken to achieve a negative margin? | Controversial. The presence of invasive carcinoma in the margin specimen is the only factor that indicates a positive margin. In many subsites, width cutoffs have been abandoned for narrow margin analysis resulting from the proximity of critical adjacent structures. |
141 | True or False. En bloc tumor resection is the only oncologically sound method for surgical management of a primary head and neck tumor. | False. Narrow-margin analysis, “bread-loafing,” or tumor mapping with frozen pathologic analysis of margins does not compromise oncologic outcomes (Hinni, 2013). |
142 | When a tumor invades a sensory or motor nerve, what is the recommended surgical approach? | Dissect proximally and distally along the nerve, take margins at either end and with the goal of obtaining negative margins on frozen section analysis. |
143 | In a patient with biopsy-proven squamous cell carcinoma metastases to the cervical lymph nodes, what are the most likely site and subsite of origin? | Unknown primary: • Site: Upper aerodigestive tract • Subsite: Oropharynx |
144 | Why is it clinically important, from both a prognostic and management standpoint, to identify the site of origin for an unknown primary tumor? | Failure to identify the site of origin results in • Significant decrease in 5-year overall survival (50%) • Need for wide-field radiation therapy with an increase in associated morbidity |
145 | What imaging modality can be helpful in identifying the unknown primary in as many as 30% of TX head and neck cancer patients? | PET/CT scan |
146 | Describe the surgical approach for a patient with an unknown primary tumor. | • Manual palpation of the upper aerodigestive tract • Visual inspection using naked-eye evaluation, rigid endoscopy, laryngoscopy and microscopy • Directed biopsies and frozen-section analysis. If negative, proceed. • Palatine and lingual tonsillectomy with frozen-section pathology ipsilateral to the cervical adenopathy. If negative, proceed. • Contralateral palatine and lingual tonsillectomy with frozen-section pathology. If negative, proceed. • Nasopharyngeal biopsies with frozen-section pathology. If negative, proceed. • Neck dissection and permanent serial sectioning of the biopsy specimens Note: If tumor is identified at any step, complete resection is advised. (Karni, 2011; Nagel, 2013). |
Overview of Radiation Therapy
147 | Why might tumor cells exposed to an increased concentration of growth factors, nutrients, and oxygen be more susceptible to radiation and chemotherapy? | A larger number will transition from G0 to G1 and enter the cell cycle, during which their DNA is more susceptible to antineoplastic therapy. |
148 | At what point during the cell cycle are cells most radiosensitive? Radioresistant? | • Radiosensitive: M phase and G2 • Radioresistant: S phase Note: The two most important checkpoints in relation to radiation damage are G1 and G2. |
149 | Does the proliferation rate of a tumor determine its radiosensitivity? | Controversial. Both proliferating and nonproliferating tissues can be radiosensitive, but the effects in nonproliferating or slowly proliferating tissues are often delayed. Radiosensitivity is unique to each tumor. |
150 | How does radiation result in cell killing? | Radiation therapy produces intracellular ionization → breaks chemical bonds, creates free radicals → DNA damage → cell death. Double-strand breaks are the most important and deadly injury imposed by radiation. |
151 | What generally determines the maximum dose of radiation that can safely be delivered to a tissue? | Ability of adjacent normal tissue to withstand the radiation and effectively repair damage |
152 | Although radiation can result in rapid cell death (apoptosis), some cells do not die until they attempt mitosis, and others continue to divide several times before cell death. What is this delayed cell killing called? | Mitotic cell death. This is why tumors do not shrink immediately after radiation and may take weeks to demonstrate the full effects of radiation treatment (simplified explanation). |
153 | Describe the basic principles involved in clinical radiobiology, which is often described as the four Rs of radiotherapy. | • Repair: Sublethal damage between fractions • Redistribution: Into radiosensitive phases of the cell cycle • Repopulation: With increased time between fractions • Reoxygenation: Response to ionizing radiation is increased 1.5–3x in well-oxygenated cells; fractionation allows for increased oxygen delivery to previously hypoxic cells. |
154 | What is the unit used to describe the absorbed radiation dose? | • Gray (Gy) = 1 Joule of energy per kilogram of material • 1 Gy = 100 centigray (cGy) = 100 rads (old unit) Note: The energy of radiation delivered determines the depth of tissue penetration. |
155 | What are the two general forms of ionizing radiation? | • Particulate: Kinetic energy is carried by a particle that has a resting mass, such as electrons, protons, or neutrons. • Electromagnetic: Massless, chargeless packets of energy (photon) that move through space at the speed of light, including X-rays and gamma rays |
156 | What are the three main radiotherapeutic modalities used clinically in head and neck cancer? | • Electrons: Produced by a linear accelerator; travel shorter distances within tissue • Photons/X-ray: Produced by linear accelerator; travel further within tissue; most widely used (e.g., intensity-modulated radiation therapy, or IMRT) • Protons: Produced by a cyclotron; charged particles; pronounced peak of energy deposition with little dose deposited beyond it (Bragg peak) Note: Can use a mix of photons and electrons |
What device accelerates electrons to a high level of energy and then allows them to (1) exit the machine as an electron or (2) collide with a specific target that results in the emission of photons (both of which can be used for treatment)? | Linear accelerator | |
158 | In what type of radiation treatment is the radiation source located outside the patient? | External-beam radiation therapy (EBRT) |
159 | What radiation strategy attempts to match the target volume (defined by high-resolution imaging, such as CT or MRI) with a high dose of radiation while limiting the amount of radiation given to adjacent normal tissue? | Conformal therapy (three-dimensional conformal radiation therapy) Note: IMRT is preferentially used to accomplish these goals in the head and neck. |
160 | What type of radiation therapy dynamically alters the intensity of radiation across a field during treatment delivery? | IMRT |
161 | What type of radiation therapy delivers a full dose of radiation in a single (or very few) fraction(s) using photons generated by a cobalt-60 source or by a linear accelerator? | Stereotactic radiation therapy, referred to as stereotactic radiosurgery for intracranial and skull base applications |
162 | What type of radiation therapy makes use of radionuclides that decay within specific anatomical subsites, resulting in very specific targeting? | Targeted radionuclide therapy (e.g., thyroid cancer and iodine-131) |
163 | Which form of radiation energy is better able to deposit most of its energy at a specific target, minimizing the dose to surrounding tissues based on the Bragg peak? | Protons |
164 | You are planning to treat a patient with a superficial head and neck cancer using photon radiation. To ensure that sufficient dose is deposited superficially, you create a material with a similar density to skin to place over the tumor. What is this called? | Bolus |
165 | What type of fractionation schedule uses radiation given in multiple daily doses without changing the overall treatment time compared with traditional daily radiotherapy, and why does this potentially result in decreased late morbidity despite a higher total dose? | Hyperfractionation. Normal tissue is more sensitive to the size of each individual dose. Therefore, if you decrease the size of each individual dose while increasing the total dose given over the entire course, there should be increase tumor cell killing and decreased impact on normal tissues. |
166 | What type of fractionation schedule relies on multiple daily treatments using larger doses of radiation and a shorter overall treatment time compared with standard daily radiation therapy? | Accelerated fractionation |
167 | What are the three primary radiosensitizing strategies currently available? | • Decreasing hypoxemia (due to increased interstitial pressure within the tumor or comorbid anemia): Hyperbaric oxygen therapy*, inhaled carbogen, hypoxic cell sensitizers (nimorazole, tirapazamine), recombinant human erythropoietin** • Concomitant chemotherapy: Additive (kills micrometastasis, toxicity profiles do not overlap) vs. synergistic effect (increased cytotoxic activity) • Targeted therapy: Goal is to decrease side effects and improve radiation efficacy; monoclonal antibody against EGFR (cetuximab). * No change in 5-year outcomes **Worse locoregional control and overall survival |
What are the five basic steps involved in radiation treatment? | • Simulation • Treatment planning (defining target volumes, imaging, dose, schedule) • Verification • Dose delivery • Quality assurance | |
169 | Imaging the patient to delineate targets and treatment volumes is done using CT or MRI. Is this typically done before or after the patient is immobilized? | After. It allows for better accuracy of treatment. |
170 | When planning radiation targets, what three volumes must be considered? | • Gross tumor volume: Delineates tumor boundaries • Clinical target volume: Identifies regions at high risk for harboring microscopic disease • Planning target volume: Includes a “margin” to allow and fraction to fraction variability in patient positioning |
171 | What types of tissues are at risk for acute radiation related toxicity? Delayed toxicity? | • Acute: Rapidly dividing cells; skin, mucous membranes, bone marrow, tumor cells. Related to total treatment time, dose per fraction, total dose, time between treatments • Delayed: More slowly dividing cells; neural and connective tissue. Related to total dose and dose per fraction |
172 | Acute radiation toxicity occurs over days to weeks following treatment. What are some of the most common toxicities associated with treatment of the head and neck? | • Mucositis • Dermatitis • Xerostomia • Hoarseness • Odynophagia • Dysphagia • Weight loss |
173 | Delayed or late radiation toxicity occurs months to years after treatment. What are the most common toxicities? | • Xerostomia • Dental caries/decay • Osteoradionecrosis, chondronecrosis • Fibrosis • Hypothyroidism • Neurologic damage |
174 | Compared with two- or three-dimensional conformal techniques, intensity-modulated radiation therapy may spare what organs within the head and neck? | • Salivary glands • Pharyngeal musculature • Otic structures • Optic structures • Temporomandibular joints (TMJs) • Brain |
175 | In an effort to reduce the incidence of osteoradionecrosis, when should decayed and nonrestorable teeth be extracted in relation to radiation therapy? | Before radiation |
176 | What are the theoretical advantages to preoperative radiation therapy? | • Reduction of unresectable tumors to the point of resectability • Reduces the extent of necessary surgery • Microscopic disease is usually more radiosensitive preoperatively because it has a better blood supply. • Cells disseminated during the course of surgery may be less viable after radiation therapy. • Requisite treatment volumes are smaller preoperatively than postoperatively. |
177 | What are the theoretical advantages to postoperative radiation therapy? | • Surgery allows for definition of the extent of tumor. • Surgery is easier before radiation. • Dosing can be adjusted depending on residual tumor after surgery. • Fewer wound-related complications |
What type of fractionation regimen has been shown to result in better local control and overall survival compared with conventionally fractionated radiation therapy? | Hyperfractionated Note: With concurrent chemoradiation therapy, there is no benefit. This is a complex issue. |
Overview of Chemotherapy
179 | What is the role of chemotherapy in the treatment of head and neck cancers? | • For patients undergoing treatment with curative intent, chemotherapy is used concurrent with radiation therapy to improve locoregional control of disease, either as definitive chemoradiation therapy or as chemoradiation therapy after complete surgical resection (adjuvant therapy). Induction chemotherapy (multidrug regimen given before definitive chemoradiation) is another accepted use of chemotherapy for head and neck cancer. • For patients with recurrent or metastatic disease not amenable to curative therapy, chemotherapy is used as a palliative treatment to help control disease and improve cancer-related symptoms. |
180 | True or False. Head and neck squamous cell carcinoma is unusually sensitive to chemotherapy for a solid tumor. | True |
181 | For squamous cell carcinoma of the head and neck, chemotherapy (5-fluorouracil [5-FU]) and cisplatin) has been demonstrated to result in overall response rates up to 90%. What percentage of patients will have complete responses, and what percentage of these complete responses can be considered a cure? | • Complete response: 20 to 50% • Cure: ~ 0%; chemotherapy cannot be used with curative intent. |
182 | Studies have shown that patients who have not been treated with prior surgery and/or radiation respond to chemotherapy almost twice as often as patients who had. What might explain this? | • Better performance status before treatment • Intact blood supply to the tumor • Prior radiation may select for clonal populations of chemo-resistant cells. |
183 | What class of chemotherapeutic agents target DNA and cause cross-linking, double-strand breaks, or substitutions, thereby interfering with DNA replication and ultimately causing mutation and/or cell death? | Alkylating agents |
184 | What inorganic platinum chemotherapeutic agent results in DNA cross-links, denaturation of strands, covalent bonds with DNA bases, and DNA intra-strand cross-links? | Cisplatin |
185 | What common side effects are associated with cisplatin administration? | Nephrotoxicity, ototoxicity, neurotoxicity, nausea/vomiting, electrolyte disturbances, myelotoxicity |
186 | Name the second-generation platinum agent that binds with DNA to create interstrand and intra-strand cross-links and protein-DNA cross-links that ultimately result in interruption of the cell cycle and apoptosis. | Carboplatin |
187 | What class of chemotherapeutic agents inhibits accurate DNA replication by imitating naturally occurring metabolites imperative to DNA replication? What are some examples? | Antimetabolites • Methotrexate: Binds to dihydrofolate reductase, which is necessary for de novo synthesis of thymidine and purine synthesis • 5-FU: Irreversibly binds to thymidylate synthetase, blocking conversion of uridine to thymidine, thereby preventing DNA synthesis |
Cultured Streptomyces spp. produce compounds that function as antibiotic chemotherapeutic agents. What agent in this class results in (1) intercalation between base pairs; (2) forms complexes with iron, thus reducing oxygen to super-oxide and hydroxyl radicals which result in DNA strand breaks; (3) DNA cross-linking, alkylation, and oxygen radicals? | Antitumor antibiotics • Doxorubicin • Bleomycin • Mitomycin | |
189 | What class of chemotherapeutic agents binds to free tubulin dimers and therefore results in disruption of microtubule polymerization or depolymerization and ultimate disruption of the cell cycle? What are some examples? | Alkaloids • Vincristine: Binds irreversibly to microtubules and spindle proteins in S phase and interferes with the mitotic spindle → arrest in metaphase • Vinblastine: Binds to tubulin and inhibits microtubule formation, disrupts mitotic spindle → arrest in M phase |
190 | What class of chemotherapeutic agents causes stabilization of microtubules, thereby inhibiting the normal cell cycle by preventing microtubule disassembly and arrest at the G2/M phase and apoptosis? What are some examples? | Taxanes • Docetaxel • Paclitaxel |
191 | What chimeric monoclonal antibody targeting EGFR, which is overexpressed in head and neck squamous cell carcinoma, has proven to be effective for this pathology? | Cetuximab |
192 | What recombinant humanized monoclonal antibody targets EGFR and is currently being investigated in head and neck cancer? | Bevacizumab |
193 | What are the potential pros and cons of induction or chemotherapy followed by definitive treatment in head and neck squamous cell carcinoma? | Pros: • Decrease the size of the tumor prior to definitive management • Increase the response to locoregional definitive management (both radiation and surgery may be more effective for smaller tumors) • Theoretically decreases the risk for distant metastases • Assess tumor response to chemotherapy (also a surrogate marker for radiosensitivity) Cons: • Difficulty identifying tumor extent • Inability to tolerate definitive management due to toxicities • Increased cost and complexity of treatment • Decreased compliance with treatment |
194 | Phase II trials demonstrated considerable promise for the use of an induction/neoadjuvant approach to head and neck squamous cell carcinoma. What were the results of subsequent phase III trials? | Controversial. Initial phase III studies demonstrated no survival advantage. However, more recent phase III trials, including agents such as docetaxel, cisplatin, and 5-FU, demonstrated both a progression-free survival and overall survival advantage (European Organization for Research and Treatment of Cancer [EORTC] 24971; TAX 324). |
195 | The Head and Neck Contracts Program, run by the National Cancer Institute, and the Head and Neck Intergroup Study 0034 both demonstrated that adjuvant chemotherapy after primary surgery or radiation has the potential to reduce what key oncologic outcome measure? | • Distant metastases • Did not impact overall survival • Can be considered “maintenance” chemotherapy |
What are some of the attributes that define high-risk disease in head and neck cancer patients that benefits from adjuvant chemotherapy? | • Positive surgical margins • Extracapsular extension • T3/T4 primary disease • Higher nodal stage • Perineural invasion • Angiolymphatic invasion • Involvement of level IV or V lymph nodes | |
197 | What is the rationale for using chemotherapy and radiation therapy together to treat head and neck squamous cell carcinoma? | Each modality functions independently from the other, but together they result in synergistic chemotherapeutic radiosensitization. |
198 | Phase III trials have demonstrated improved disease-free survival for patients undergoing adjuvant chemoradiation therapy for high-risk disease. What factors conferred a high-risk status for these studies? | • Positive surgical margins • Extracapsular extension |
199 | Which agents have shown a survival advantage for concurrent chemotherapy as single agents? | • Cisplatin (low-dose daily; high-dose every 3 weeks) • Carboplatin • 5-FU |
200 | Aggressive, multiagent chemotherapy has been added to radiation therapy for head and neck cancer and has resulted in a locoregional control rate in some studies of > 90%. In this cohort of patients, what is the most likely oncologic failure? | Distant metastases. May suggest a role for induction chemotherapy. Note: Controversy is ongoing as to whether the benefit of multiagent chemotherapy outweighs the risks. Therefore, single-agent chemoradiation therapy remains the standard of care for this approach. |
201 | What clinical outcome has driven research into definitive chemoradiation strategies for head and neck cancer? Name two studies that provided evidence to uspport this approach. | Organ preservation Department of Veterans Affairs Laryngeal Cancer Study Intergroup Radiation Oncology Group (RTOG) 91–11 |
Neck Anatomy
202 | How are the lymph node levels divided in the neck? ( | They are separated into levels based on anatomic or surgical and radiographic criteria. The following are the most commonly involved groups: • Level I (IA/IB)
• Level II (IIA/IIB)
• Level III: Middle jugular chain • Level IV: Lower jugular chain • Level V (VA/VB): Posterior triangle
• Level VI: Anterior jugular chain |
 IA: Submental triangle
IA: Submental triangle IB: Submandibular triangle
IB: Submandibular triangle IIA: Upper jugular chain
IIA: Upper jugular chain IIB: Submuscular recess
IIB: Submuscular recess VA: Spinal accessory chain
VA: Spinal accessory chain VB: Supraclavicular and transverse cervical chain
VB: Supraclavicular and transverse cervical chain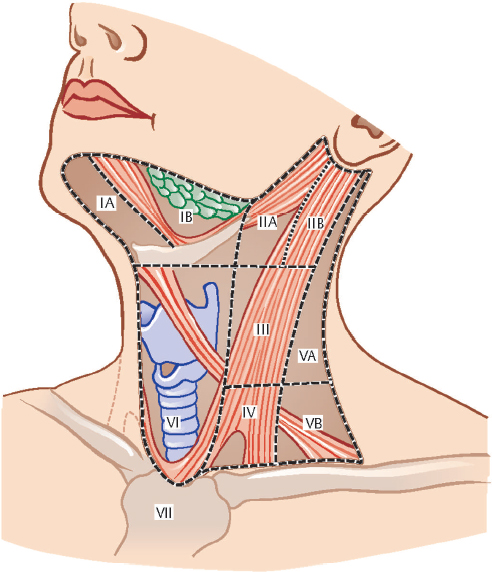
203 | In addition to the six nodal levels, there are additional, unclassified nodal groups that are important in the surgical management of the neck. What are these, and where are they found? | • Suboccipital nodes: Deep to the insertion of the trapezius muscle • Retroauricular nodes: Superficial postauricular region • Parotid nodes: Can be superficial to, within or deep to the parotid gland • Retropharyngeal nodes: Between the prevertebral fascia and the pharyngeal constrictor muscles • Facial nodes: Superficial and deep to the facial artery and vein |
204 | What lymph node levels in the neck are unpaired? | Level IA. Level VI is often considered to have a right and a left but may also be considered as a single compartment. |
205 | How is level IB distinguished from level IIA surgically and radiographically? | Posterior edge of the submandibular gland |
206 | How is the lateral border of level IIA defined radiographically? | Posterior border of the internal jugular vein |
207 | What anatomical structure divides lymph node level II into IIA and IIB surgically? | Spinal accessory nerve (CN XI) |
208 | How are the superior and inferior boundaries of level IIA surgically defined? | • Superior: Skull base • Inferior: Carotid bifurcation |
209 | What are the radiographic and surgical landmarks that separate neck levels II and III? | Inferior border of the hyoid bone (radiographic) and carotid bifurcation (surgical) |
What are the superior and inferior borders of level III radiographically? | • Superior: Horizontal plane from the inferior border of the hyoid bone • Inferior: Horizontal plane from the inferior border of the cricoid cartilage | |
211 | What are the radiographic and surgical landmarks that separate neck levels III and IV? | Inferior border of the cricoid cartilage (radiographic) and the omohyoid muscle (surgical) |
212 | What anatomical structure divides lymph node level V into VA and VB? | A horizontal plane from the inferior border of the cricoid cartilage Note: Level VA includes the spinal accessory nodes, VB includes the transverse cervical nodes and supraclavicular nodes. Just inferior to the clavicle lies the sentinel node or Virchow node. |
213 | What are the surgical landmarks that define level VI (central compartment) lymphatics? | Hyoid bone superiorly, suprasternal notch inferiorly, and common carotid arteries laterally |
214 | Level VI lymph nodes are at greatest risk for metastasis from which primary locations? | • Glottic and subglottic larynx • Pyriform sinus • Cervical esophagus • Thyroid gland |
215 | What are the major divisions of cervical fascia in the neck? | • Superficial cervical fascia • Deep cervical fascia: Superficial (investing), middle (visceral), and deep layers |
216 | What layer of cervical fascia covers the superficial surface of the platysma muscle and is continuous with the superficial muscular aponeurotic system (SMAS) superiorly in the face and fascia overlying the chest, shoulder, and axilla? | Superficial cervical fascia |
217 | Which layer of cervical fascia arises from the vertebral spinous processes, wraps around the SCM and trapezius muscles, covers the mylohyoid muscle and anterior bellies of the digastric muscle, attaches to the hyoid bone, forms the floor of the submandibular and posterior triangle, wraps around the submandibular gland and parotid glands, and splits at the mandible into the internal layer, which lies over the medial surface of the medial pterygoid muscle and inserts onto the skull base, while the outer layer passes over the masseter muscle and inserts onto the zygomatic arch? | Superficial (investing) layer of the deep cervical fascia |
218 | What are the two subdivisions of the middle layer of the deep cervical fascia? | • Muscular division: Surrounds infrahyoid strap muscles, attached superiorly to the hyoid bone and thyroid cartilage and inferiorly to the sternum • Visceral division: Surrounds the thyroid, trachea, and esophagus and extends into the mediastinum to connect with the fibrous pericardium. Superiorly, the fascia may blend with the buccopharyngeal fascia (controversial). |
219 | Name the fascial layers that line the inner (pharyngeal) and outer (cervical) surface of the pharyngeal constrictor muscles. | • Inner: Pharyngobasilar fascia • Outer: Buccopharyngeal fascia |
220 | What are the two named divisions of the deep layer of the deep cervical fascia? | • Prevertebral fascia: Fused to the transverse processes of the vertebral bodies with extension medially to cover the prevertebral musculature and vertebral bodies. Continues posteriorly to cover the extensor muscles and insert onto the vertebral spinous processes • Alar fascia: Located between the prevertebral fascia and the visceral division of the middle layer of the deep cervical fascia |
What layer(s) of cervical fascia form the carotid sheath? | The superficial (investing), middle (visceral), and deep layers of the deep cervical fascia | |
222 | What is enveloped by the superficial (investing) layer of the deep cervical fascia? | • Two muscles (SCM and trapezius) • Two glands (parotid and submandibular gland) • Two spaces (Posterior triangle, suprasternal space of Burns) |
223 | What is the vascular supply and innervation of the platysma muscle? | • Innervation: Cervical branch of the facial nerve (CN VII) • Arterial supply: Submental branch of the facial artery and suprascapular artery |
224 | The SCM extends from the mastoid process of the temporal bone to the clavicle and manubrium, where it inserts as two separate heads (medial/sternal and lateral/clavicular) forming the lesser supraclavicular fossa. What is the innervation and blood supply to this muscle? | • Innervation: Spinal accessory nerve (CN XI), ventral rami of C2–4 • Arterial supply:
|
225 | Describe the innervation and arterial supply to the anterior and posterior bellies of the digastric muscle. | • Innervation
• Arterial supply
|
226 | Name the four paired infrahyoid strap muscles in order from superficial to deep. | • Superficial: sternohyoid and omohyoid • Deep: sternothyroid and thryohyoid |
227 | What is the predominant innervation and vascular supply to the infrahyoid strap musculature? | • Innervation: Ansa cervicalis (C1–3) • Arterial supply: Superior thyroid artery and lingual artery |
228 | What muscle can be found in the lateral neck extending from the transverse processes of C3 through C6 to the first rib, passing just posterior to the phrenic nerve, just anterior to the subclavian artery, and just medial to the brachial plexus? | Anterior scalene muscle |
229 | What spinal nerves provide sensory innervation to the cervical skin? | Ventral rami of C2–4 from the cervical plexus • Lesser occipital nerve (C2): Posterior scalp and ear • Great auricular nerve (C2, C3): Anterior branch → skin over parotid gland; posterior branch → mastoid area, lower ear and lobule • Transverse cutaneous nerve (C2, C3): Ascending/descending branches → anterolateral neck skin • Supraclavicular nerve (C3, C4): Medial, intermediate and lateral (posterior) branches → supraclavicular skin from second rib to shoulder |
230 | What anatomical location describes the point where the cutaneous nerves of the cervical plexus exit posterior to the sterncleidomastoid muscle, and what is the relationship between this point and the spinal accessory nerve (CN XI)? | Erb’s point The spinal accessory nerve (CN XI) passes approximately 1 cm superior and deep to the sternocleidomastoid muscle and Erb’s point. |
231 | What are the muscular branches that constitute the cervical plexus? | • Phrenic nerve (C3–5) • Inferior branch of ansa cervicalis (C1–3) • Segmental branches including cervical branches of the spinal accessory nerve (C1–4) |
What structure travels deep to the deep cervical fascia and superficial to the anterior scalene and can be found when dissecting levels III and IV? | Phrenic nerve (C3–5) | |
233 | The submandibular duct passes between what two nerves? | Lingual nerve and hypoglossal nerve |
234 | The sympathetic trunk travels deep and medial to the carotid sheath and is just superficial to the prevertebral fascia and what muscle? | Longus colli |
235 | What structure branches off the vagus nerve (CN X) at approximately T1–2, wraps around the subclavian artery from anterior to posterior, ascends in the neck along the tracheoesophageal groove, generally posterior to the inferior thyroid artery, and enters the larynx at a 30- to 45-degree angle by passing under the inferior constrictor muscle and through the cricothyroid joint space? | Right recurrent laryngeal nerve |
236 | The left recurrent laryngeal nerve wraps around the aortic arch before passing superiorly in the neck in the tracheoesophageal groove to enter the larynx at a 0- to 30-degree angle by passing under the inferior constrictor muscle and through what laryngeal space? | Cricothyroid |
237 | Describe the classic relationship between the inferior thyroid artery and the recurrent laryngeal nerve. | • 50%: Nerve passes deep to artery. • 25%: Nerve passes between arterial branches. • 25%: Nerve passes anterior to artery. Note: This relationship is extremely variable and may not represent a reliable landmark for identifying the nerve. |
238 | What is the incidence of a right nonrecurrent inferior/recurrent laryngeal nerve? | 0.5 to 1% |
239 | What anomaly is associated with a right aberrant retroesophageal subclavian artery? Situs inversus? | • Right nonrecurrent inferior/recurrent laryngeal nerve • Left nonrecurrent inferior/recurrent laryngeal nerve |
240 | What structure is formed by the anastomoses of the posterior (dorsal) recurrent laryngeal nerve fibers and the posterior (dorsal) fibers of the internal branch of the superior laryngeal nerve, and what is its function? | Galen anastomosis (aka ramus anastomaticus) |
241 | What artery branches from the aortic arch, passes over the trachea from left to right and branches into the right common carotid artery and right subclavian artery? | Innominate (brachiocephalic) artery |
242 | What are the major divisions of the right subclavian artery? | • First part: Right, from innominate artery just posterior to the sternoclavicular joint to the medial border of the anterior scalene muscle; may rise 2 cm above the clavicle. Left, from aortic arch at T3–4 to the medial border of the anterior scalene muscle • Second part: Highest point, spans the width of the anterior scalene muscle. • Third part: Lateral border of anterior scalene muscle to outer border of the first rib → axillary artery |
What artery branches off the first part of the subclavian artery, ascends in the neck by passing through the foramina of the transverse processes of C1–C6, and enters the foramen magnum and joins with its paired contralateral vessel to form the basilar artery? | Vertebral artery | |
244 | What are the three arteries that arise from the first part of the subclavian artery? | • Vertebral artery • Thyrocervical trunk • Inferior thoracic artery |
245 | Name the branches of the thyrocervical trunk that branch off the first part of the subclavian artery at approximately the medial border of the anterior scalene muscle? | • Inferior thyroid artery • Suprascapular artery • Superficial/transverse cervical artery |
246 | On the left, the costocervical trunk arises from the first part of the subclavian artery, and on the right it arises from the second part. To what vessels does it give rise? | • Deep cervical artery • Superior intercostal artery |
247 | What structures are contained within the carotid sheath? | • Carotid arteries: Medial • Internal jugular vein: Lateral • Vagus nerve: Posterior |
248 | At what vertebral level(s) is the carotid bifurcation in the majority of people? | C3–4 (~ at the level of the superior border of the thyroid cartilage) |
249 | What bony skull base structure runs between the internal and external carotid arteries? | Styloid process |
250 | What are the branches of the external carotid artery, and to what named branches do these arteries give rise? ( | • Superior thyroid artery → infrahyoid, superior laryngeal, cricothyroid and sternocleidomastoid arteries • Ascending pharyngeal artery → pharyngeal, inferior tympanic, and meningeal arteries • Lingual artery → suprahyoid, dorsal lingual, and sublingual arteries • Facial artery → ascending palatine, tonsillar, submental and glandular arteries • Occipital artery → Upper and lower branches to the sternocleidomastoid muscle • Posterior auricular artery → stylomastoid artery • Internal maxillary artery → see below • Superficial temporal artery → frontal and parietal branch |
 Occipital and posterior auricular arteries
Occipital and posterior auricular arteries Superior thyroid artery
Superior thyroid artery Suprascapular artery
Suprascapular artery Anterior: mylohyoid branch of the inferior alveolar nerve (CN V3)
Anterior: mylohyoid branch of the inferior alveolar nerve (CN V3) Posterior: facial nerve (CN VII)
Posterior: facial nerve (CN VII) Anterior: submental branch of the facial artery
Anterior: submental branch of the facial artery Posterior: posterior auricular and occipital arteries
Posterior: posterior auricular and occipital arteries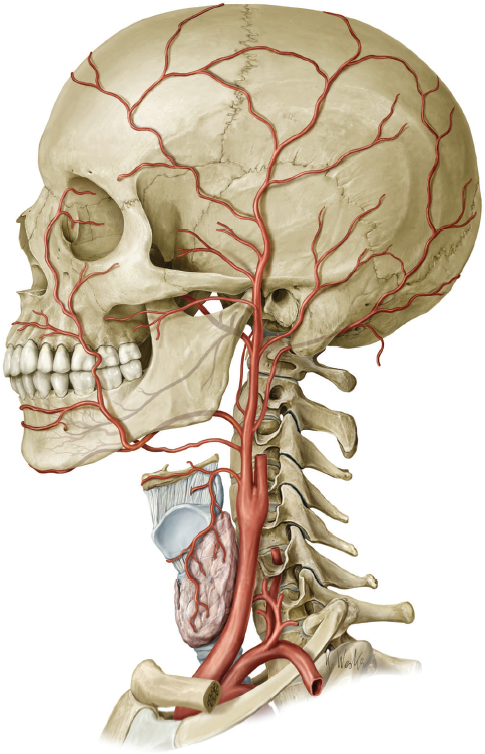
251 | What artery arises at the level of the greater cornu of the hyoid bone from the external carotid, runs deep to the posterior belly of the digastric muscle and stylohyoid muscle, turns at the middle constrictor to follow the posterior boundary of the submandibular gland and medial border of the medial pterygoid muscle, and then winds around the mandible at the level of the facial notch? | Facial artery |
252 | What artery, or branch of this artery, often transverses level IIB in the neck and “tethers” the hypoglossal nerve in level IIA? | Occipital artery |
253 | What are the three parts of the internal maxillary artery? | • First part/mandibular portion: Arises between the ramus of the mandible and the sphenodmandibular ligament, passes the posterior to the lateral pterygoid muscle • Second part/pterygoid portion: Within the lateral pterygoid muscle • Third part/pterygopalatine portion: Pterygopalatine fossa |
What are the branches of the first part (mandibular portion) of the internal maxillary artery? | • Deep auricular artery • Anterior tympanic artery • Middle meningeal artery • Accessory meningeal artery • Inferior alveolar artery • Mylohyoid artery | |
255 | What are the branches of the second part (pterygoid part) of the internal maxillary artery? | • Anterior deep temporal artery • Posterior deep temporal arteries • Pterygoid branches • Masseteric artery • Buccinator/buccal artery |
256 | What are the branches of the third part (pterygopalatine part) of the internal maxillary artery? | • Posterior superior alveolar artery • Infraorbital artery • Sphenopalatine artery • Artery of the pterygoid (vidian) canal • Pharyngeal artery |
257 | What sensory organ(s) is located at the bifurcation of the common carotid artery, and what is the innervation? | • Carotid sinus → internal carotid artery, baroreceptor, glossopharyngeal nerve (IX), vagus nerve (X), sympathetics • Carotid body → posterior or between the carotid bifurcation, chemoreceptor, same innervation |
258 | What veins give rise to the external jugular vein, what structures does it drain, and where does it drain into? | • Retromandibular vein and postauricular vein • Scalp and face • Subclavian vein |
259 | What superficial veins drain the anterior neck by emptying into the external jugular vein or the subclavian vein and are at risk during thyroidectomy and tracheostomy? | Anterior jugular veins |
260 | What structures exit the skull base through the jugular foramen with the internal jugular vein? | Glossopharyngeal nerve (IX), vagus nerve (X), accessory nerve (XI), inferior petrosal sinus, and internal jugular vein |
261 | The internal jugular vein drains most of the head and neck into what venous structure? | Subclavian vein → brachiocephalic vein |
262 | What structure most commonly passes from the superior mediastinum, through the thoracic inlet on the left into level IV, passing anterior to the phrenic nerve and anterior scalene muscle, posterior to the carotid sheath, and most commonly terminates at the confluence of the left subclavian vein and internal jugular vein? | Thoracic duct |
263 | What is the incidence of right-sided thoracic duct in the neck? Bilateral? | • Right-sided only: 4% • Bilateral thoracic ducts: 12 to 15% |
Evaluation and Management of the Neck
264 | Malignancies involving the neck primarily arise as metastatic lesions (most commonly from the upper aerodigestive tract). What percentage of neck malignancies will arise primarily in the neck, and what are the most common sites of origin? | 15%. Thyroid, salivary gland, and lymphoma |
265 | What percentage of neck masses in pediatric patients are benign? | > 90%, most commonly inflammatory |
266 | Approximately what percentage of neck masses in adult patients are neoplastic? | ~ 80% |
267 | What is the most common head and neck malignancy in the pediatric population and the second most common head and neck malignancy in the adult population after squamous cell carcinoma? | Lymphoma |
What are common sites of origin for locoregional metastatic disease to cervical lymph nodes? | • Upper aerodigestive tract • Head and neck skin • Major and minor salivary glands • Thyroid gland | |
269 | What are the most common sites of origin for distant metastatic disease to cervical lymph nodes? | • Lung • Thoracic esophagus • Ovary • Prostate • Kidney |
270 | What is the most likely site of origin for squamous cell carcinoma metastatic to cervical lymph nodes with an unknown primary? | Oropharynx (tonsil and tongue base) |
271 | What are the most common symptoms associated with nodal metastases to the neck? | • Palpable neck mass • Symptoms resulting from compression (e.g., dysphagia, dysphonia) • Symptoms resulting from invasion (e.g., recurrent laryngeal nerve paralysis, accessory neuropathy, pain) |
272 | What is the most common anterior neck mass diagnosed on physical examination? | Thyroid nodule |
273 | What are important features of lymphadenopathy that can be detected on a careful physical examination? | • Location • Mobility on palpation and with swallowing • Potential deep involved structures • Firm (i.e., not rubbery) • Involvement of the skin |
274 | True or False. Nodal cervical metastases from locoregional tumors are generally extremely painful. | False |
275 | When malignant lymphadenopathy is immobile and invasion or adherence of the nodal disease to underlying structures is suspected, what is the neck referred to as, and what implications does this have on management? | Fixed. It may be unresectable. |
276 | What is the best diagnostic test for determining the cause of a neck mass without a known primary tumor? | FNA biopsy |
277 | What diagnostic test is indicated if an FNA biopsy is performed on a suspicious cervical lymph node with an unknown primary and the pathology demonstrates lymphoid cells? | Excisional lymph node biopsy, most commonly in the operating room |
278 | Although there has been a significant amount of research into the application of sentinel lymph node biopsy for head and neck cancer, currently the literature supports its routine use for what types of cancer? | Cutaneous malignancies (especially melanoma). May also be used for known oral cavity cancer in patients with cN0 neck disease. |
279 | What are the general steps involved with performing a sentinel lymph node biopsy? | • Primary tumor is injected with technetium-99 sulfur colloid in the radiology suite. • Lymphoscintigraphy is performed, and the sentinel node is identified. • Patient is brought to the operating room (generally within 4 hours). • Use the gamma probe to confirm the location of the sentinel node and design surgical incision. • Slowly inject ~ 0.3 mL of isosulfan blue intradermally (not subcutaneously). This should result in a lacelike pattern under the skin. This should be done at least 10 minutes before any local anesthetic is injected if any is injected at all. • Expose the tissue suspected of harboring the sentinel lymph node. • Using the gamma probe (pointing away from the primary site if possible to avoid shine-through), identify the area containing the node. Visual confirmation of a blue node is supportive but not required if the gamma probe is suggestive. • Excise the node and perform a 10-second gamma count in the dissection field to confirm that the sentinel node(s) was (were) removed. • With the node placed away from the primary site and sentinel biopsy site, perform a confirmatory gamma count for 10 seconds to ensure you have removed the correct node. • Excise the primary with appropriate margins. This may be done first if the primary is in close proximity to the sentinel lymph nodes. • Depending on the pathology report results, the wound can be closed or a formal neck dissection is performed. Note: It is not unusual for multiple lymph nodes to be identified. If the dissection bed after sentinel node excision contains > 10% of the gamma count detected before the node was removed, further exploration for remaining nodes is warranted. |
280 | In patients with common carotid artery or internal carotid artery invasion with tumor, which test should be employed before surgical resection of the involved carotid artery? | Carotid artery balloon occlusion test |
281 | What imaging modality is most commonly used for the initial workup of an adult neck masses? | CT with contrast |
282 | What imaging modality is best for evaluation of perineural spread associated with neck masses? | MRI |
283 | What imaging modality is best used to determine distant metastatic spread of disease and as an adjunct in patients with an unknown primary tumor? | PET/CT |
284 | What is the AJCC node (N) staging system for head and neck cancer (including salivary gland; excluding nasopharynx and thyroid)? | • Nx: Regional lymph nodes cannot be assessed • N0: No regional lymph node metastases • N1: One lymph node involved ≤ 3 cm • N2a: One ipsilateral lymph node involved > 3 cm and ≤ 6 cm in size • N2b: More than one ipsilateral involved lymph node, none > 6 cm • N2c: Contralateral or bilateral lymph node involvement ≤ 6 cm • N3: Lymph node > 6 cm |
285 | What is the AJCC lymph node (N) staging system for nasopharyngeal cancer? | • Nx: Regional lymph nodes cannot be assessed. • N0: No regional lymph node metastases • N1: Unilateral metastases in one of more lymph node ≤ 6 cm, above the supraclavicular fossa • N2: Bilateral metastases in lymph nodes ≤ 6 cm, above the supraclavicular fossa • N3a: Tumor > 6 cm • N3b: Tumor extends to the supraclavicular fossa. |
286 | What is the AJCC lymph node (N) staging system for soft tissue sarcomas? | • Nx: Regional lymph nodes cannot be assessed. • N0: No regional lymph node metastases. • N1: Regional lymph node metastases |
What is the AJCC lymph node (N) staging system for thyroid cancer? | • Nx: Regional lymph nodes cannot be assessed. • N0: No regional lymph node metastases Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|