21 Head and Neck Cancer in the Elderly
 Prevalence of Head and Neck Cancer among the Elderly
Prevalence of Head and Neck Cancer among the Elderly
The definition of elderly continues to evolve as human lifespans increase. The National Institute of Aging and the National Institutes of Health use three categories to define aged patients: 65 to 74 years as young old, 75 to 84 years as older old, and 85 and over as oldest old.1 A chronological landmark is considered the age of 70, because an increased incidence of age-related physiological changes becomes present at this age, resulting in pharmacokinetic changes that may lead to increased treatment-related toxicity.2 Although aging is associated with a variety of declining physiological functions, due to the fact that biological age may differ greatly from chronological age, thorough evaluation and risk assessment are needed for decision making in the setting of head and neck cancers. It is imperative for the treating physicians to consider the factors that might affect a patient’s ability to withstand cancer treatment. In addition, it is important to estimate the life expectancy of a patient when treatment strategies are planned. In Western societies, age-adjusted life expectancy is ~ 13.6 years for a 70-year-old man and 16.4 years for a 70-year-old woman.2
Head and neck cancers occur within the paranasal sinuses, nasal cavity, oral cavity, pharynx, and larynx. In 2014, there were an estimated 55,070 new cases of head and neck cancers, with 12,000 head and neck cancer-related deaths in the United States.3 Worldwide, head and neck cancer is the sixth most common cancer, with roughly 650,000 new cases reported annually. Despite the increasing prevalence of cancer related to the human papillomavirus, which primarily affects younger patients,4,5 head and neck cancer remains principally a cancer of an older population. According to the Surveillance, Epidemiology, and End Results database, ~ 47% of all patients diagnosed with head and neck cancer in the United States between 1973 and 2008 were age 65 and older.6 In addition, the incidence of newly diagnosed head and neck cancer cases among the elderly is expected to increase by more than 60% by the year 2030.7
In the realm of head and neck cancer, squamous cell carcinoma of the head and neck (SCCHN) is the most prevalent and challenging malignancy to treat and is thus the focus of discussion. The treatment for SCCHN has become quite complex, necessitating multidisciplinary teams and multimodality therapy. Historically, tumors of the head and neck have been treated primarily with open surgery–alone approaches. The use of postoperative adjuvant radiation therapy (RT) became common in the 1970s, although its introduction in SCCHN began several decades earlier. Mounting data subsequently followed demonstrating that adjuvant treatment with RT improved locoregional control rates, thus improving overall survival. Further investigations have also led to the use of RT alone for the primary treatment of certain early-stage SCCHN with excellent outcomes. Along with surgery and RT, a third efficacious modality to treat SCCHN is chemotherapy. Investigated most thoroughly in the last decades of the 20th century, chemotherapeutic regimens, as a neoadjuvant therapy or in combination with RT in the postoperative setting, have shown great promise as an adjunct therapy in further improving oncological outcomes. In the mid to late-1990s, concomitant chemoradiation therapy (CRT) became a viable primary treatment option for certain patients with advanced-stage SCCHN. Yet, despite the continued advances in the therapeutic options available for SCCHN patients over the past 20 or more years, overall survival (OS), disease-free survival (DFS), functional outcomes, and toxicity profiles from therapy have remained relatively poor.8 To date, patients with SCCHN continue to have some of the lowest survival rates of all major cancer types.
In the era of multimodality therapy, treatment paradigms for older patients with head and neck cancer are not well defined. The majority of patients with head and neck cancer will present with advanced (stage III and IV) disease requiring multimodality therapy.9 Combined surgery, radiation, and chemotherapy cause significant acute toxicity and long-term morbidity, thus reducing compliance to therapy and decreasing quality of life as well as life expectancy. These morbidities can be profound in older patients, secondary to comorbid medical conditions and impaired functional status. As a result, older patients are often considered poor candidates for multimodality treatment and are therefore less likely to receive standard of care therapy compared with younger patients.10,11 This bias against optimal treatment in the elderly may jeopardize their chance of cure. A retrospective series from Ortholan et al noted deviation from institutional protocol for head and neck cancer treatment in greater than half of older patients.12 Although standardized treatment plans should be based on clinical stage and prognosis, age-related comorbidities and frailty need to be taken into account. Healthy older patients should be treated as aggressively as younger patients,13 and treatment plans should be adapted in higher-risk frail elderly patients to balance the goal of curative treatment with an increased risk of treatment-related morbidity and mortality.12
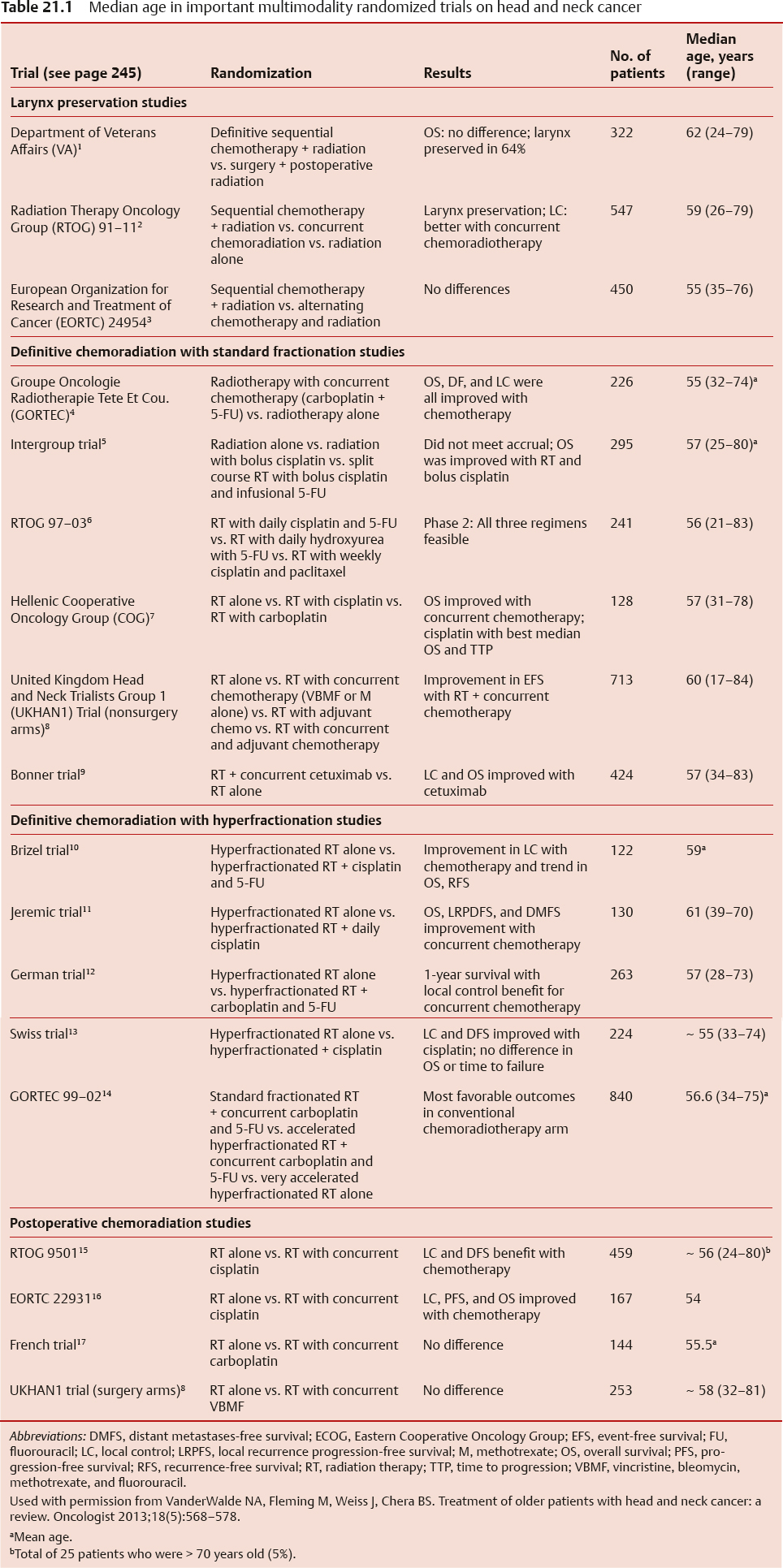
In addition, older patients are often ineligible for the large prospective, randomized trials14 on which treatment paradigms are based (Table 21.1). For example, in a recent meta-analysis of 93 clinical trials, only 692 of 17,346 patients (4%) were ≥ 70 years of age.15 Thus the outcomes of these studies may not be applicable to older patients. Despite recommendations not to include age limits in large prospective trials, many ongoing trials continue to have upper age limits in their inclusion criteria.
Limited data suggest that selected older patients have survival outcomes similar to younger patients when treated primarily with surgery. In particular, several retrospective studies have matched older patients to a younger cohort and have shown no difference in survival outcome.16–18 One study matched 115 patients who were ≥ 70 years of age by tumor type and stage to 115 patients < 70 years of age and found no difference in 5-year survival rate.16 In addition, multiple nonmatched retrospective studies have shown similar results.19,20
An integral component of treatment planning is access to a Head and Neck Tumor Board Conference. Once a cancer diagnosis is confirmed, optimal treatment strategies are designed and individualized during a multidisciplinary tumor board. A multidisciplinary approach to patients has been shown to alter diagnosis, stage, and treatment modalities in head and neck cancer patients in nearly a third of patients.21 Change in treatment was significantly more common in cases of malignancy, occurring in 24% of patients versus 6% of benign tumors. Significant changes in treatment were also noted to be largely escalations in management by incorporating multimodality therapy.21 Furthermore, discussion at a multidisciplinary head and neck tumor conference may serve as a forum to mitigate bias that continues to surface in the literature regarding the elderly patient population with respect to treatment stratification.
 Quality of Life Assessment and Comorbidities
Quality of Life Assessment and Comorbidities
The challenge in identifying surgical candidacy in the elderly population begins with preoperative quality of life assessment. Quality of life is a multidimensional concept that includes evaluation of positive and negative aspects of life.22 Quality of life refers to “a patient’s appraisal of and satisfaction with their current level of functioning compared with what they perceive to be possible or ideal.”23 There is limited quality of life data available in older head and neck cancer patients. The reason for this is unclear; however, subjective evaluation using validated quality of life questionnaires may be especially challenging in older patients. Treating physicians quite often believe that older patients have more side effects and toxicities from treatment and have more difficulty adjusting to their cancer diagnosis, thus overestimating the problems faced by their older patients with cancers and potentially affecting the aggressiveness of care.24
Although preconceived notions regarding the disproportionate impact of surgical therapy in the elderly persist, several studies have demonstrated no differences in posttreatment quality of life between older and younger head and neck cancer patients. A prospective assessment of surgically treated patients with head and neck cancer studied quality of life at 3 months postoperatively and observed no age-based differences.25 An institutional database analysis of quality of life in 289 patients with head and neck cancer stratified by sex and age determined that, although global quality of life assessments are predicted by age, head and neck–specific metrics are not.26 This is supported by a similar analysis using head and neck–specific quality of life instruments.27 These findings were further confirmed in a long-term prospective observational study demonstrating that age did not impact on the quality of life for up to 6 years after diagnosis.28
Interestingly, younger patients may report worse quality of life outcomes after treatment for head and neck cancer. In a prospective study comparing quality of life, 78 older patients and 105 younger patients with head and neck cancer undergoing surgery were stratified based on baseline changes in physical function.27 Although older patients had worse physical functioning prior to treatment, the difference remained constant throughout treatment, indicating that the older patients did not have a higher relative decrease in physical functioning compared with younger patients.27 In addition, younger patients reported more pain at 6 months than older patients.27 This difference is not limited to physical performance only, given that one retrospective study of 638 patients demonstrated that patients older than 65 had better long-term physical and emotional functioning than younger patients following surgery.29 These findings may suggest that older patients experience fewer quality-of-life difficulties than their younger peers. Alternatively, they may suggest that older patients are less likely to report changes in quality of life due to differences in perceived expectations. Although the current data suggest that older patients do not have worse quality of life following treatment, the subjective nature of quality-of-life end points makes it difficult for clinicians to interpret these data for their individual older patients.
Another important preoperative assessment in the elderly is a careful evaluation of medical comorbidities. One case-control study did not identify significant differences in postoperative complications, mortality, or recurrence in a diverse population of patients with head and neck cancer stratified by the age of 70 who were treated surgically.16 Despite data suggesting that age itself does not influence outcomes in head and neck cancer,30 it stands to reason that patients with medical comorbidities and poorer functional reserve (common issues in older patients with SCCHN) would experience more and/or worse treatment-related toxicity.
The literature on head and neck cancer surgical outcomes stratified by medical comorbidities reveals mixed and conflicting conclusions. In one retrospective evaluation, medical comorbidities, independent of age, did independently predict postoperative complications.31 Another demonstrated an increase in 30 day postoperative mortality in older patients (3.5% mortality) as compared with that in a younger cohort (0.8%).32 However, the authors here concluded that, given the relatively low rate of perioperative mortality, age alone should not be a contraindication to aggressive surgery. In a large retrospective analysis of 310 patients over age 70 with mucosal and salivary head and neck cancers, the authors determined that medical comorbidities (measured on the Adult Comorbidity Evaluation-27 index, see Appendix) and performance status (using the Karnofsky performance scale [Table 21.2]), as well as age > 80, all independently predict survival.33 Finally, another study limited to patients > 80 years of age indicated that age did not impact on survival in early-stage disease but was a strong predictor of poor overall survival (median, 8 months) in patients with advanced-stage cancer.34
A new paradigm to emerge in the evaluation of candidacy for treatment may be defined not by age but by frailty. In a population study of 61,740 elderly patients,35 frail elderly is defined as 66 years of age or older with comorbidity scores of 2 or higher and was examined as an independent variable in an analysis that included the previously described independent variables as well as acute medical complications, surgical complications, dysphagia, and weight loss as dependent variables.17 Frail elderly status was additionally examined as an independent variable in analyses of short-term mortality, surgical complications, acute medical complications, length of stay, and costs that included an interaction term between frail elderly status and weight loss. The median age in this study was 73 years (range, 66–104 years) and did not differ significantly between groups based on comorbidity status; however, patients 80 years of age or older were more likely to have advanced comorbidity. Cardiovascular diseases and chronic pulmonary disease were the most frequent comorbidities and had an increased prevalence in patients with advanced comorbidity scores.35
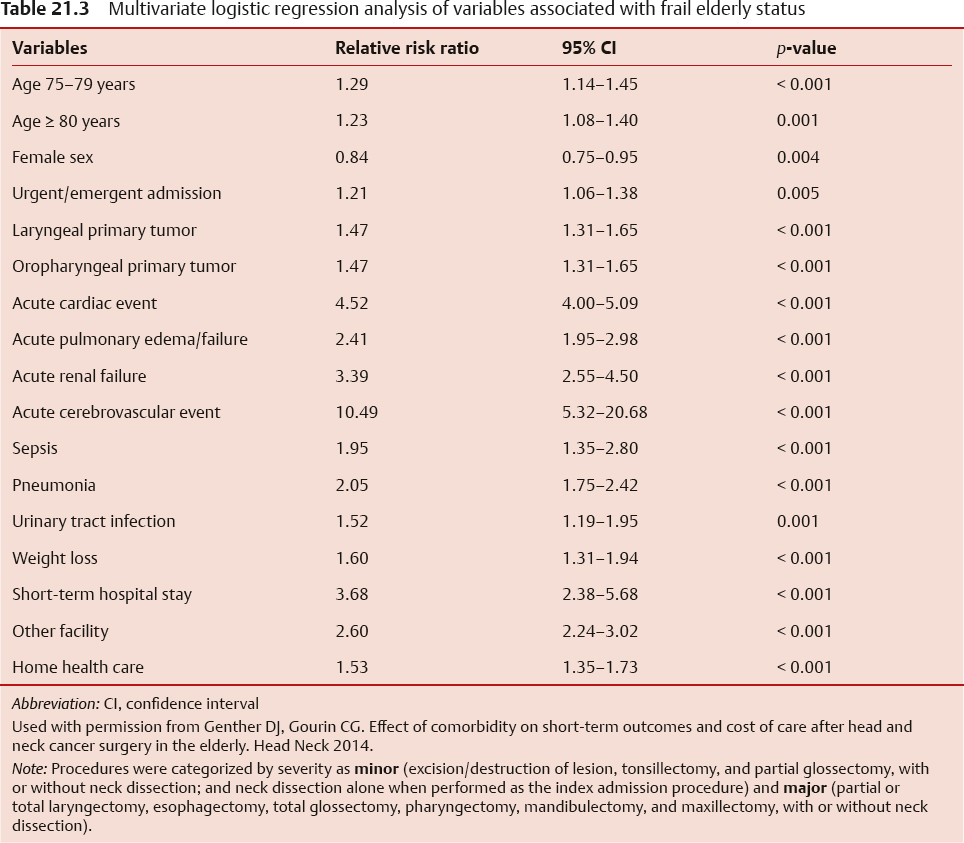
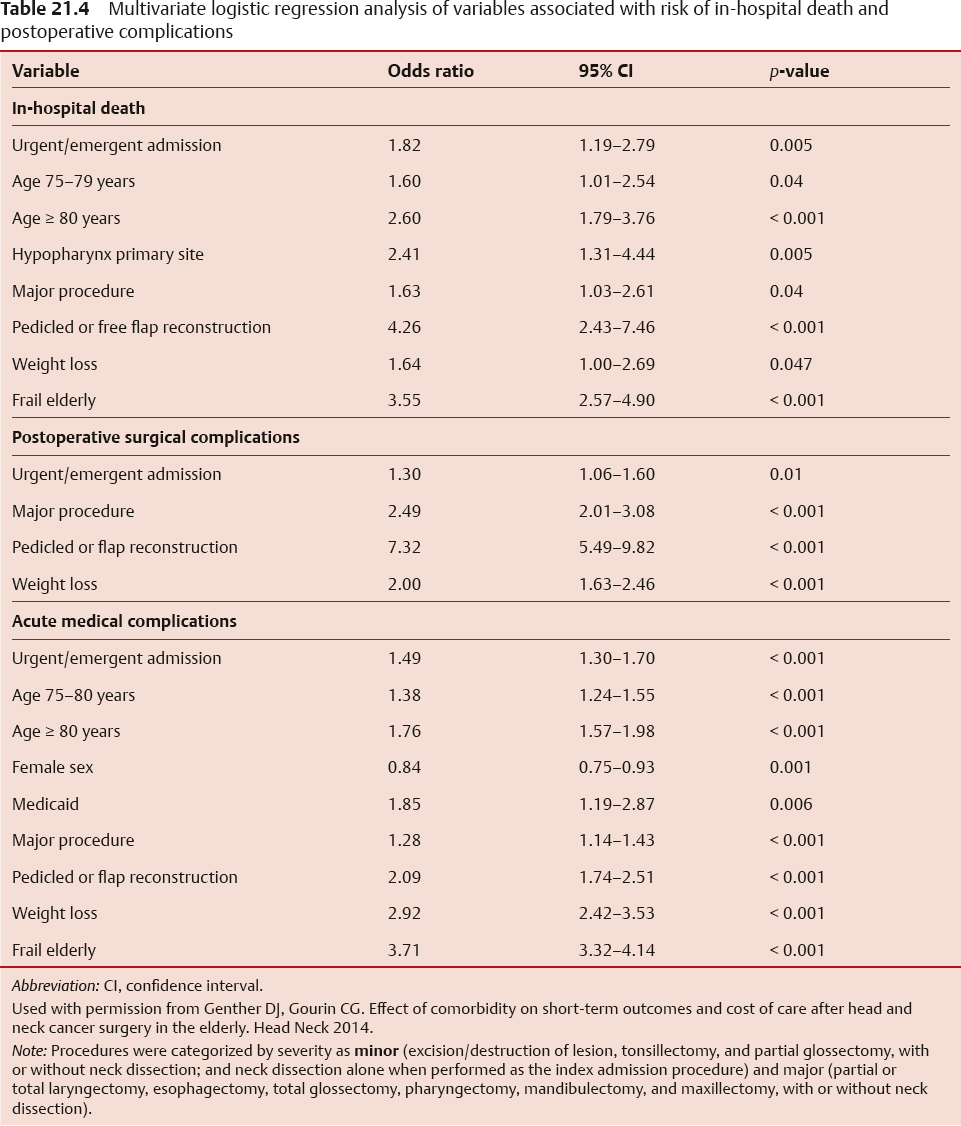
Multinomial regression analysis was performed to identify variables associated with frail elderly patients, identifying a cohort that was significantly more likely to be 75 years of age or older, required urgent admission, and had significantly increased risks of acute medical complications (Table 21.3). Multiple logistic regression analyses of independent variables associated with the risk of in-hospital death and complications are shown in Table 21.4. After controlling for the effects of all variables, statistically significant independent predictors associated with the risk of in-hospital death were urgent or emergent admission, age 75 years or older, hypopharyngeal primary site disease, procedure, pedicled or free flap reconstruction, weight loss, and frail elderly status. Postoperative surgical complications were significantly associated with urgent or emergent admission, major procedure, pedicled or free flap reconstruction, and weight loss, but not frail elderly status. Finally, acute medical complications were significantly associated with frail elderly status, age 75 years or older, urgent or emergent admission, major procedure, flap reconstruction, and weight loss.35 Although the data presenting are conflicting, the evidence favors a comprehensive treatment approach in patients with head and neck cancer, with appropriate modifications in those with multiple comorbidities, which may assist surgical planning and help take preventive measures to minimize potential complications.
Table 21.2 Karnofsky performance scale status definitions rating (%) criteria
Able to carry on normal activity and to work; no special care needed | 100 | Normal to no complaints; no evidence of disease |
| 90 | Able to carry on normal activity; minor signs or symptoms of disease. |
| 80 | Normal activity with efforts; some signs or symptoms of disease |
Unable to work; able to live at home and care for most personal needs; varying amount of assistance needed. | 70 | Cares for self; unable to carry on normal activity or to do active work |
| 60 | Requires occasional assistance but is able to care for most of personal needs |
| 50 | Requires considerable assistance and frequent medical care |
Unable to care for self; requires equivalent of institutional or hospital care; diseases may be progressing rapidly | 40 | Disabled; requires special care and assistance |
| 30 | Severely disabled; hospital admission is indicated although death not imminent |
| 20 | Very sick; hospital admission necessary; active supportive treatment necessary |
| 10 | Moribund; fatal processes progressing rapidly |
| 0 | Dead |
Used with permission from Oxford Textbook of Palliative Medicine, Oxford University Press; 1993:109. | ||
 Factors to Consider in Surgical Procedures for Elderly
Factors to Consider in Surgical Procedures for Elderly
Preoperative Nutrition
Nutrition in the elderly is often impaired without the acute or chronic impacts that the presence of a head and neck cancer would create. Alterations in the senses of smell and taste as well as social isolation often create a relative anorexia with diminished caloric intake. This combined with decreased activity leads to a loss of lean body mass. In the setting of SCCHN, the presence of malnutrition plays a vital role in wound healing.
Preoperative consideration of how to deliver adequate nutrition must be addressed given that one of the three phases of swallowing will be affected after surgical intervention. A study evaluating nutrition impact symptoms, defined as key determinants of reduced dietary intake, weight loss, and reduced functional capacity of patients with head and neck cancer before treatment, suggests that symptoms before treatment may adversely affect nutritional intake, weight/body mass index (BMI), and the functional capacity of patients with head and neck cancer.36 Diagnosis, management, and treatment of symptoms were essential in preventing weight loss. To do this, patients must be assessed for nutrition impact symptoms (NISs), such as dysphagia, mouth sores, xerostomia, dental problems, and difficulty chewing. The extent of dysphagia is graded from 0 to 4, from no dysphagia (grade 0) up to dysphagia for all kinds of oral intake including liquids (grade 4).
A patient-generated subjective global assessment tool (PG-SGA)37 was used to systematically collect information on the NISs of the patients, and linked to dietary intake and weight loss. The PG-SGA is a validated nutritional screening technique for patients with cancer, which includes NIS, dietary intake, height, weight, weight loss history, and functional capacity. A PG-SGA score ≥ 9 indicates a higher nutritional risk, and in this report 31% of patients fell into this category.36
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


