and Charles P. Molumi2
(1)
University of Papua New Guinea and Port Moresby General Hospital, Boroko, National Capital District, Papua New Guinea
(2)
Port Moresby General Hospital, Boroko, National Capital District, Papua New Guinea
10.1 Excision of Lipoma Over Parotid Region
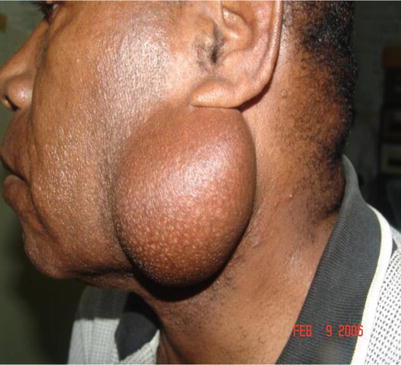
Fig. 10.1
Parotid lipoma before excision
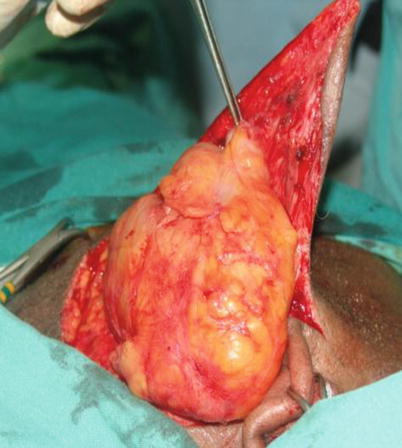
Fig. 10.2
Raising the flap at the subcutaneous tissue level exposed the lipoma. It is easily excised by staying very close to the tumor

Fig. 10.3
The specimen is removed and sent for histopathological examination, a penrose drain inserted and wound closed

Fig. 10.4
A penrose drain is inserted and the wound closed
10.2 Excision of Sebaceous Cyst
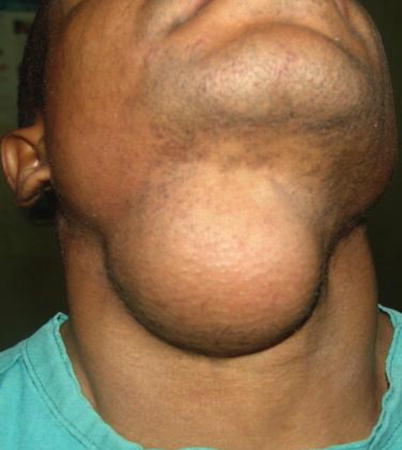
Fig. 10.5
Submandibular sebaceous cyst before excision

Fig. 10.6
The skin flap is raised at the subcutaneous tissue plane exposing the cyst. Tissue attachments around the capsule are excised and the cyst removed

Fig. 10.7
The intact specimen with intact capsule is removed and examined

Fig. 10.8
The cyst opened exposing the sebaceous contents
10.3 Excision of Parapharyngeal Neurofibrosarcoma

Fig. 10.9
Incision is marked out for mandibulotomy and inclusion of previous surgical scar for excision with the tumor
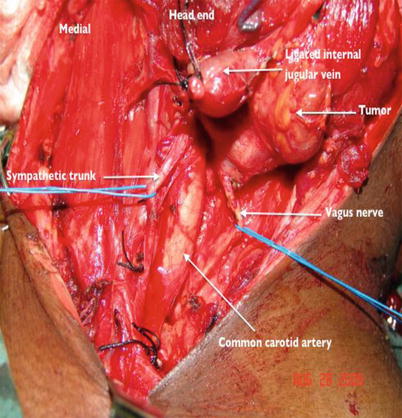
Fig. 10.10
After mandibulotomy as described in Chap. 7, the entire tumor is exposed together with the neurovascular structures. The external jugular vein is ligated as it is involved by the tumor. The tumor is found to be arising from the vagus nerve
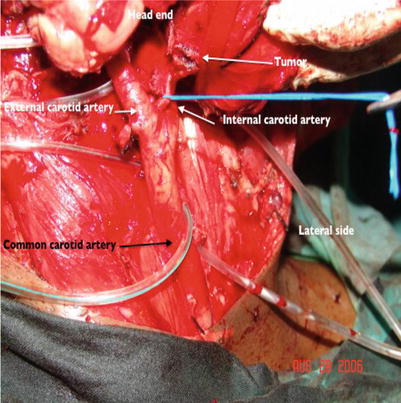
Fig. 10.11
The tumor is dissected away from the common carotid artery and followed to the angle of the mandible
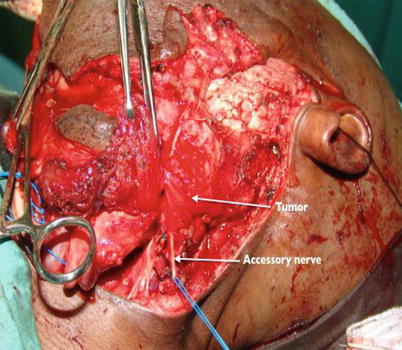
Fig. 10.12
Dissection at the lateral border of the tumor shows involvement of the accessory nerve
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


