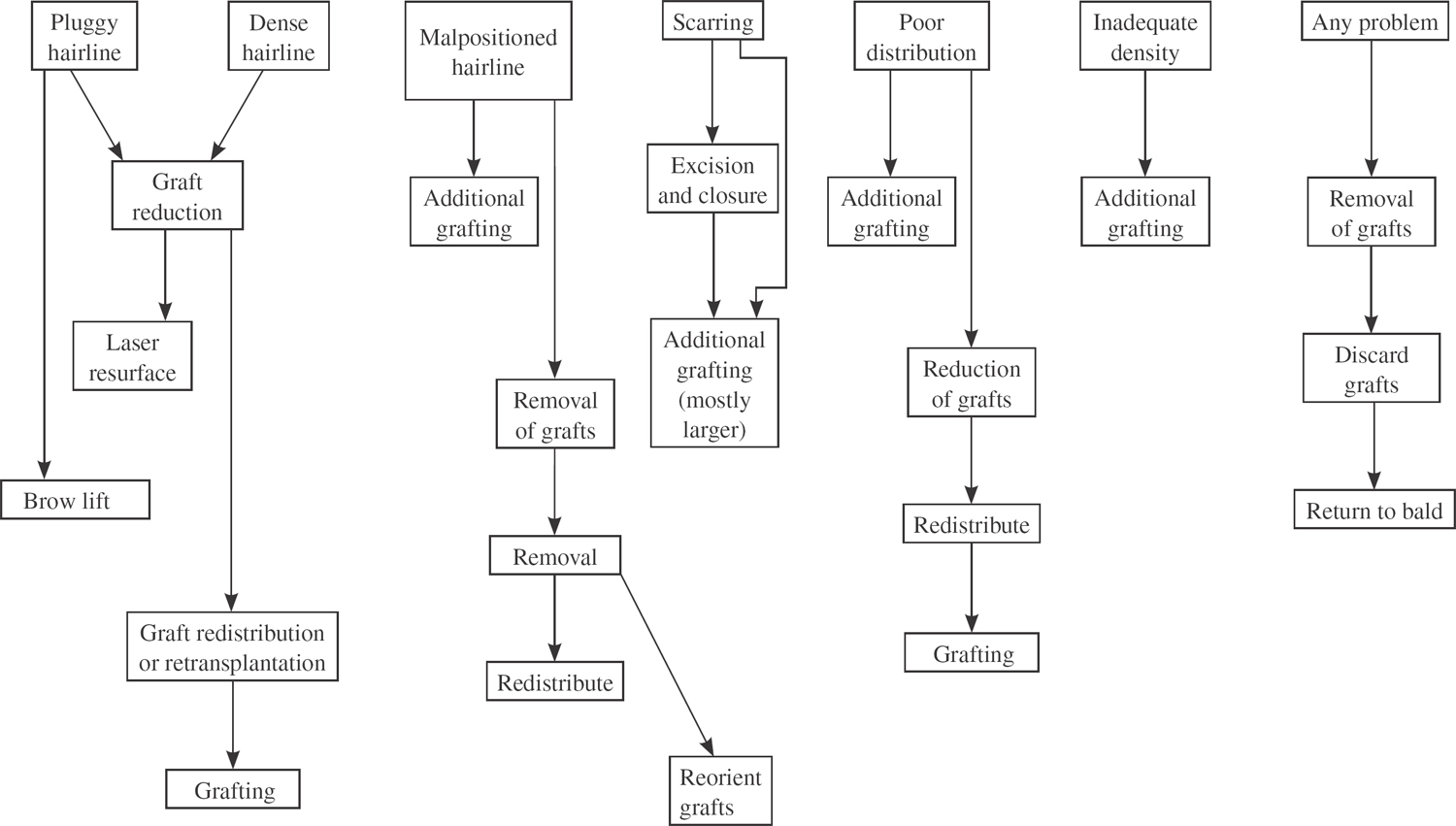
35 Hair Replacement and Revision Surgery In a practice devoted to hair restoration, a considerable percentage of individuals presenting for treatment are those who have had prior procedures and are seeking to improve appearances. For this 30% of the practice’s patients, the goals are sometimes as high as expressed by those with virgin scalps (a completely undetectable restoration), but for the majority of revision surgery patients, the goals are somewhat tempered (a less detectable restoration). And for the overwhelming majority of revision surgery patients, in fact it is possible to overcome the limitations incurred by less than optimal work and significantly improve appearances. An understanding of the evolution of hair transplantation provides a framework on which to evaluate the results from prior procedures and to decide upon a course of treatment. Since the early days of hair transplantation, beginning in the late 1950s in the United States with the use of large plug grafts, the evolution of techniques has been toward the goal of achieving undetectability. Although the current technique follicular unit grafting is indicated in most hair restorations performed today, in some revision cases the final result may best be achieved using more conventional techniques, but incorporating some of the technical aspects of follicular unit grafting. Hair transplantation involves the surgical moving of “permanent” hairs from one part of the scalp to areas of baldness or hair thinning, and remains the only “permanent” treatment for male and female pattern hair loss, not curing the process but improving upon its manifestations. Several other conditions are also treatable with hair transplantation, the most common being alopecic scarring from prior surgical or other trauma. In the original technique of plug grafting, the graft consisted of a 3 to 4 mm circle of scalp containing as many as 20 hairs. When punched out from the back of the scalp and placed into a similarly sized hole in the front or other part of the scalp, some or most of the hairs from the graft grow. Because hair does not naturally grow in groups of 15 or more hairs, plug grafting results in an unnatural appearance best described as doll’s hair. Other problems with plug grafting include scarring in the donor area and the often poor growth of the transplanted hairs. Another significant problem is scarring of the skin surrounding the grafts. Most commonly presenting as hypopigmentation and/or hypertrophic scarring, it is a result of the large amount of skin transplanted along with the hairs. Improved aesthetic outcomes from plug grafting relied upon staged procedures, usually three to four, performed at 4-month intervals, to fill in all surrounding areas, essentially creating a solid wall of hair. The total amount of bald scalp that could be covered using this solid coverage technique was limited, leaving the scalp behind the solid hairline to be bald or transplanted with spread-out plug grafts. At its best, plug grafting provided coverage that relied on careful hair grooming. At its worst, the patient looked as if he had doll’s hair. More natural-appearing results became possible with the use of smaller grafts. Dividing a 4 mm plug graft in half or quarters, or using 3 and 2 mm punches for graft harvesting, created minigrafts containing four to eight hairs. Appearances certainly improved with these smaller grafts, which relied less on the creation of a solid wall and more on a spread-out distribution. Micrografts, small grafts typically containing one or two hairs, when placed in front of the minigrafts along the hairline significantly improved results. Their use, which was popularized in the early 1990s, permitted the creation of a softer, more natural-appearing hairline.1 Improvements in appearance came not only through the use of smaller grafts. Techniques of donor site harvest improved with several innovations, including suturing of the punch graft sites (facilitated by the excision of the skin between the individual punch graft holes), which evolved into the harvesting of the donor tissue as a single strip rather than individual punches. This single strip, no more than 10 to 12 mm wide and easily reapproximated with a simple running suture, remains the technique of choice. Enhanced appreciation of the aesthetics of hair transplantation evolved as well. Recognition of the proper direction and position of hair growth significantly improved appearances. Developments in hairline design, the scope of which is beyond the content of this chapter, but which is nicely reviewed in the literature,2 and more anteriorly angled direction of grafts are two of the more important areas of improvement. But perhaps no advancement in hair transplantation was more important than the recognition of the lifetime progressive nature of male pattern hair loss. With this knowledge, the responsible hair transplant physician could better plan the restoration and counsel for the possible need for more transplantation in the future. Decision tree for revision hair restoration Today, the culmination of advancements in hair transplantation has produced what nearly all leading hair transplant surgeons agree is the state-of-the-art technique, follicular unit grafting.3 This technique relies on microscopic dissection to create grafts, each containing a single follicular unit. The follicular unit, as described originally by Headington, is the naturally occurring grouping of one to four hairs, most commonly two or three hairs, and the supporting glandular elements, surrounded by a fine adventitial sheath.4 The use of the microscope is required to more accurately identify the individual follicular units, and to remove all the non-hair-bearing tissue (which can constitute as much as 50% of the total donor tissue). Although it is a technically demanding procedure, requiring a team of trained assistants to dissect and assist in the planting of as many as 3500 grafts, the natural results justify the effort. The advantages of follicular unit grafting are many, most due to the smaller size of the grafts. Because the recipient sites are smaller, they can be placed closer together to maximize density, while minimizing trauma to already existing hairs in the areas being transplanted. In addition, healing is quicker, and there is minimal to no scalp scarring in the areas of the transplanted hair. Other advantages include less trauma to the hair follicles during graft dissection, resulting in as much as a 20% greater growth of hair, and more accuracy in dividing grafts by the number of hairs they contain, therefore assuring the placement of only one hair graft along the anteriormost hairline. But the most important advantage of the technique is that, because the grafts contain hairs as they grow naturally in the scalp, the results are the most natural. This explains why follicular unit grafting is the procedure of choice for most of the leading hair transplant surgeons in North America. Individuals seeking reparative procedures present with a variety of concerns and problems with the results from prior transplants. Often the patient simply complains of “unnatural appearances,” while other times identifying the reason for dissatisfaction with the transplant. It is the job of the revision hair transplant surgeon to both identify the problem(s) and counsel the patient as to what can realistically be achieved. Given the disappointment these patients feel with the results of prior procedures, it is critical to reestablish trust in the doctor–patient relationship. The following is a review of the most common indications for performing revision surgery. • Pluggy hairline: the classic “doll’s hair” appearance, with the hairline composed of large grafts with intervening non-hair-bearing scalp • Dense hairline: similar to the pluggy hairline, except that multiple procedures were performed of usually large grafts to create a solid wall of hairs. Commonly, the density decreases significantly just a few centimeters behind this hairline. • Malposition of the hairline: including several situations, often occurring simultaneously: • Inadequate frontotemporal recessions: a flat or broad hairline, which in its extreme can create a simian appearance due to the caudal position of the lateral hairline • Asymmetric hairline: whereby one side of the hairline is lower than the other, giving an off-balance appearance • Too low a hairline: commonly seen when the hair transplant had been performed on a young man, at which time a lower hairline seemed appropriate, but with advancement in age that hairline is inappropriately low. These too low hairlines often create challenges of filling in the remainder of the scalp (see Poor Distribution of Transplants). • Misdirection of hair growth: one of the more common errors, usually the result of recipient incisions made at a more perpendicular angle, rather than the cosmetically appropriate more anterior acute angle. This is a problem almost inherent in plug grafts because of the difficulty in making larger punches at a sharp angle, but it often occurs with slit grafting. Besides looking less natural, the more perpendicular direction of hair growth results in a coarser appearance that is the result of the human eye looking at the base of the transplanted hair shafts, a phenomenon avoidable when the hairs grow in the viewer’s direction. • Scarring of the recipient scalp: fibrosis, cobblestoning, ridging, and altered pigmentation of the recipient site are forms of scarring that largely result from the skin of the graft that gets transplanted along with hairs. Healing of large grafts is often associated with scar formation, sometimes resulting in hyperfibrosis and ridging.5 Larger grafts, especially plug grafts, but even conventional micro- and minigrafts where a large cuff of skin is often present, are at high risk of causing these forms of scarring. • Poor distribution of transplants: because of poor planning for the progression of hair loss, older transplant procedures often used many of the donor hairs, not leaving enough donor hairs to cover areas of further hair loss. One result is a fully transplanted crown region that with further hair loss leads to the development of a cuff or halo of bald scalp around the crown transplants with not enough donor hairs available to further transplant and extend the area covered. Another problem can be the result of transplanting into the frontotemporal recessions, creating in the future with further hair loss a bald central forelock surrounded by filled-in frontotemporal recessions. Typically, it is those areas that lose hair later in the balding process that are the most critical to transplant to achieve a natural-appearing restoration. • Inadequate density: probably the most common complaint of patients transplanted with modern techniques. This is usually the result of insufficient or deceptive pre-op counseling. Unrealistic expectations of density leave the patient dissatisfied. Poor growth of transplanted hairs can also result in a less than anticipated density. Rough handling and desiccation of grafts are two of the most common reasons believed to result in this poor hair growth.
A Relevant History of Hair Transplantation
Indications for Revision Surgery
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Ento Key
Fastest Otolaryngology & Ophthalmology Insight Engine
