Chronic granulomatous inflammation is a proliferative inflammation characterized by a cellular infiltrate of epithelioid cells [and sometimes inflammatory giant cells, lymphocytes, plasma cells, polymorphonuclear leukocytes (PMNs), and eosinophils; see Chapter 1]. I. SO (Figs 4.1 and 4.2) is a bilateral, diffuse, granulomatous, T-cell-mediated uveitis that occurs from two weeks to many years after penetrating or perforating ocular injury and is associated with traumatic uveal incarceration or prolapse. B. Removal of the injured eye before sympathetic uveitis occurs usually completely protects against inflammation developing in the noninjured eye.1 Once the inflammation starts, however, removal of the injured (“exciting”) eye probably has little effect on the course of the disease, especially after 3–6 months. II. Blurred vision and photophobia in the noninjured (sympathizing) eye are usually the first symptoms. Vision and photophobia worsen concurrently in the injured (exciting) eye, and a granulomatous uveitis develops (see Fig. 4.1A). III. The cause appears to be a delayed-type hypersensitivity reaction of the uvea to antigens localized on the retinal pigment epithelium or on uveal melanocytes. A. The lymphocytic infiltrate consists almost exclusively of T lymphocytes. B. B cells found in some cases, usually of long duration, may represent the end stage of the disease. IV. Histologically, SO has certain characteristics that are suggestive of the disorder but not diagnostic. A. Sympathetic uveitis is a clinicopathologic diagnosis, never a histologic diagnosis alone. B. The following four histologic findings are characteristic of both sympathizing and exciting eyes: 2. Sparing of the choriocapillaris. 3. Epithelioid cells containing phagocytosed uveal pigment. 4. Dalen–Fuchs nodules (i.e., collections of epithelioid cells lying between Bruch’s membrane and the retinal pigment epithelium with no involvement of the overlying neural retina and sparing of the underlying choriocapillaris).2 1. Tissue damage caused by the trauma 2. Extension of the granulomatous inflammation into the scleral canals and optic disc I. Phacoanaphylactic endophthalmitis (PE) (Fig. 4.3) is a rare, autoimmune, unilateral (sometimes bilateral if the lens capsule is ruptured in each eye), zonal, granulomatous inflammation centered around lens material. It depends on a ruptured lens capsule for its development. II. The disease occurs under special conditions that involve an abrogation of tolerance to lens protein. III. Histologically, in addition to the findings at the site of injury, a zonal granulomatous inflammation is found. D. Usually the iris is encased in, and inseparable from, the inflammatory reaction. I. Cytomegalic inclusion disease (salivary gland disease; Fig. 4.4) B. Clinically, a central retinochoroiditis, as seen in the congenital form, is similar to that seen in toxoplasmosis. 2. Neural retinal detachments may develop in 15% of affected eyes. 3. Other ocular findings include iridocyclitis, punctate keratitis, and optic neuritis. C. Histologically, a primary coagulative necrotizing retinitis and a secondary diffuse granulomatous choroiditis are seen. II. Varicella/herpes zoster virus (VZV; Figs 4.5 and 4.6) A. VZV causes varicella (chickenpox) and herpes zoster (shingles). 2. Congenital infection is rare (differential diagnosis consists of the TORCH syndrome; see Chapter 3). 3. In immunocompetent individuals, VZV is a major cause of the acute retinal necrosis syndrome (see Chapter 11). B. Ocular complications occur in approximately 50% of cases of herpes zoster ophthalmicus: 2. Anterior segment: iridocyclitis followed by peripheral anterior synechiae, exudate, and hyphema I. Tuberculosis (Mycobacterium tuberculosis; Figs 4.7 and 4.8) B. Tubercle bacilli reach the eye through the bloodstream, after lung infection. D. Histologically, the classic pattern of caseation necrosis consists of a zonal type of granulomatous reaction around the area of coagulative necrosis. II. Leprosy (Hansen’s disease; M. leprae; Fig. 4.9) 2. Histologically, a diffuse type of granulomatous inflammatory reaction, known as a leproma, is present. b. The lepra cells and Virchow’s cells teem with beaded bacilli (no immunity). B. In tuberculoid leprosy, the lepromin test is positive, suggesting immunity. The prognosis is good. 3. Histologically, a discrete (sarcoidal, tuberculoidal) type of granulomatous inflammatory reaction is seen, mainly centered around nerves. III. Syphilis (Treponema pallidum; Fig. 4.10) A. Both the congenital and acquired forms of syphilis may produce a nongranulomatous interstitial keratitis (see Chapter 8) or anterior or posterior uveitis. Syphilis may occur in immunologically deficient patients (e.g., those with AIDS). B. Syphilis, a venereal disease, is divided into three chronologically overlapping stages. 2. Secondary stage: The period when the systemic treponemal concentration is greatest, usually 2–12 weeks after contact. a. This stage may be manifest by fever, malaise, lymphadenopathy, and mucocutaneous lesions. b. The secondary stage subsides in weeks to months but may recur within 1–4 years. C. The common form of posterior uveitis is a smoldering, indolent, chronic, nongranulomatous inflammation. 2. A more virulent type of uveitis may occur with a granulomatous inflammation. 1. The chronic nongranulomatous disseminated form of posterior choroiditis: 2. The granulomatous form of posterior chorioretinitis: b. Spirochetes can be demonstrated in the inflammatory tissue. 3. The preceding two types of reactions may also involve the anterior uvea. IV. Lyme disease (Borrelia burgdorferi; Fig. 4.11) C. Like syphilis, Lyme disease is divided into three chronologically overlapping stages. Not all patients exhibit each stage, and the signs and symptoms are variable within each stage. 2. Stage 2 occurs within days, weeks, or even months and reflects systemic dissemination of the spirochete. 3. Stage 3 can follow a disease-free period and may last years. a. “Lyme arthritis” is the hallmark of stage 3, appearing in more than 50% of untreated cases. c. Ocular findings include stromal keratitis, episcleritis, orbital myositis, and cortical blindness. V. Streptothrix (Actinomyces; Fig. 4.12) A. The organism responsible for streptothrix infection of the lacrimal sac (see Chapter 6) and for a chronic form of conjunctivitis belongs to the class Schizomycetes, which contains the genera Actinomyces and Nocardia. The organism superficially resembles a fungus, but it is a bacterium, best classified as an anaerobic and facultative capnophilic bacterium of the genus Actinomyces. VI. Cat-scratch disease [CSD: Bartonella (previously called Rochalimaea) henselae, cat-scratch bacillus] A. CSD is a subacute regional lymphadenitis following a scratch by a kitten or cat (or perhaps a bite from the cat flea, Ctenocephalides felis), caused by the cat-scratch bacillus, B. henselae, a slow-growing, fastidious, gram-negative, pleomorphic bacillus, which is a member of the α2 subgroup of the class Probacteria, order Rickettsiales, family Rickettsiaceae. 2. Ocular findings include Parinaud’s oculoglandular fever (see Chapter 7), neuroretinitis, branch retinal artery or vein occlusion, multifocal retinitis (retinal white-dot syndrome), focal choroiditis, intraretinal white spots, macular hole, optic disc edema associated with peripapillary serous retinal detachment, optic nerve head inflammation, and orbital infiltrates. C. The domestic cat and its fleas are the major reservoir for B. henselae. D. Histopathologically, the characteristics are discrete granulomas (which in time become suppurative) and follicular hyperplasia with general preservation of the lymph node architecture. 1. Warthin–Starry silver stain demonstrates the cat-scratch bacillus in tissue sections. 2. Electron microscopy shows extracellular rod-shaped bacteria. VII. Tularemia (Francisella tularensis, also called Pasteurella tularensis; Fig. 4.13)
Granulomatous Inflammation
Introduction
Post-Traumatic
Sympathetic Uveitis [Sympathetic Ophthalmia (SO), Sympathetic Ophthalmitis]
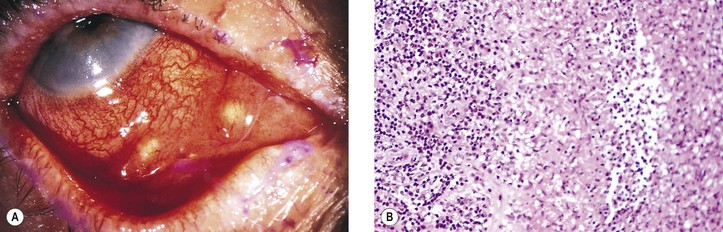
Phacoanaphylactic (Phacoimmune, Phacoantigenic, or Phacogenic) Endophthalmitis
Nontraumatic Infections
Viral
Bacterial
The nonvenereal treponematoses caused by subspecies T. p. pertenue (yaws) and T. p. endemicum (bejel) are morphologically indistinguishable from T. pallidum and display only subtle immunologic differences.

Granulomatous Inflammation
4
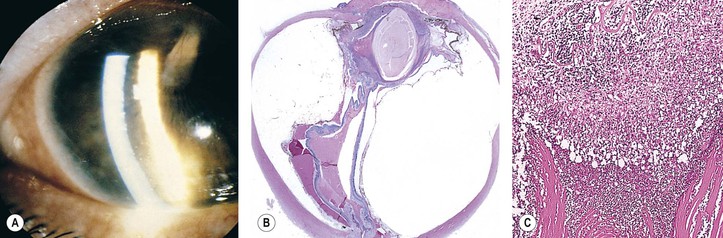
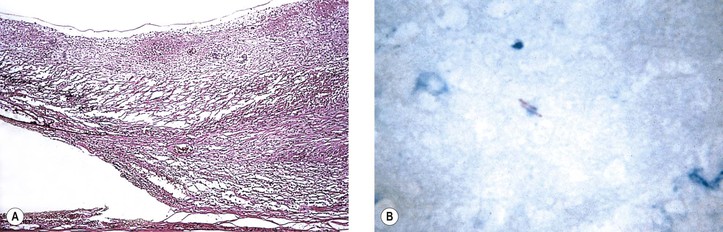
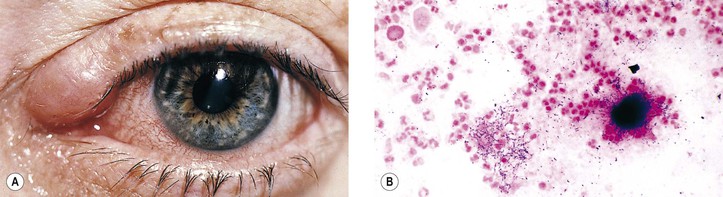
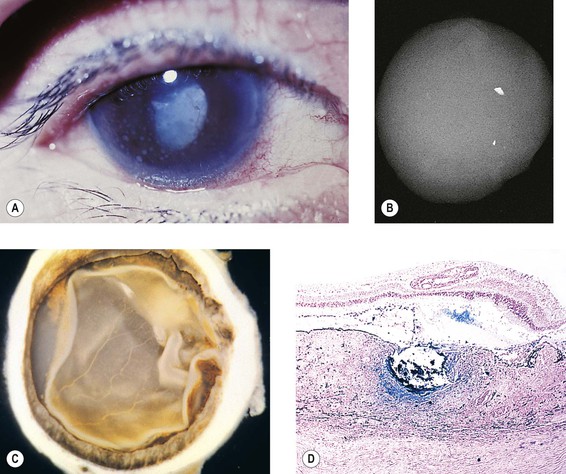
Fig. 4.1 Sympathetic uveitis. A, Large, “greasy,” mutton-fat keratic precipitates (KPs: collections of epithelioid cells, lymphocytes, and plasma cells on posterior surface of cornea) seen in patient with sympathetic uveitis. B, Another patient had a perforating injury to his eye. The other (sympathizing) eye developed photophobia and mutton-fat KPs; the injured (exciting) eye was enucleated. Radiograph of enucleated eye shows two metallic foreign bodies in eye. C, Gross specimen shows massive, diffuse thickening of choroid. D, Granulomatous inflammation fills and thickens the choroid (see also Fig. 4.2A and B). The Perl stain is positive (blue) for iron in the large, dark foreign body in the choroid. (B–D, Courtesy of Dr. TH Chou.)
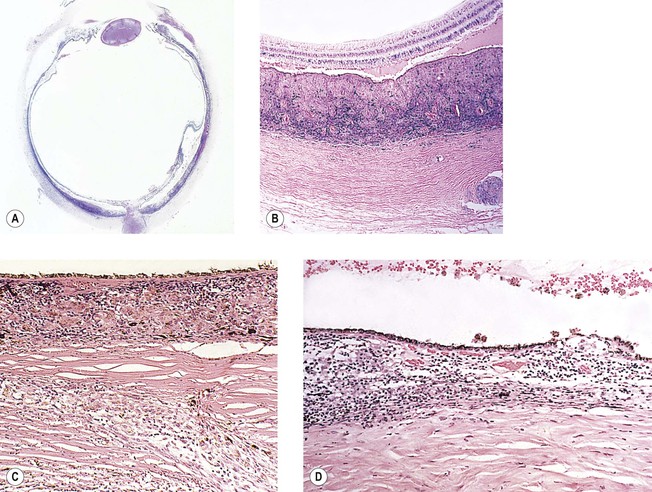
Fig. 4.2 Sympathetic uveitis. A, Enucleated eye from Fig. 4.1B and C shows diffuse thickening of the choroid (shown with increased magnification in B) by granulomatous inflammation. The pale areas represent epithelioid cells, and the dark areas consist mainly of lymphocytes. C, Sparing of the choriocapillaris and pigment phagocytosis by epithelioid cells is seen. Note granulomatous inflammation of scleral canal in lower right corner (reason why evisceration does not protect against sympathetic uveitis). D, Dalen–Fuchs nodule of epithelioid cells between retinal pigment epithelium and Bruch’s membrane is seen. Underlying choriocapillaris is spared, and overlying neural retina is free of inflammatory process. (Courtesy of Dr. TH Chou.)