Fig. 10.1
The Koeppe lens (Courtesy of Ocular Instruments Inc. Bellevue, Washington)
Direct lenses are used to perform surgical procedures involving the iridocorneal angle, such as goniotomy. The Hoskins-Barkan (Fig. 10.2) and Swan-Jacobs (Fig. 10.3) lenses are commonly used. These lenses can also be used to examine sedated or anesthetized patients, either at the operating microscope or with a portable slit lamp, replacing the need for the Koeppe lens (Fig. 10.4).

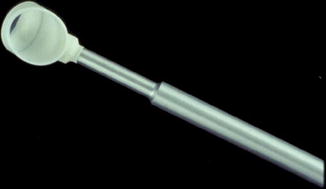
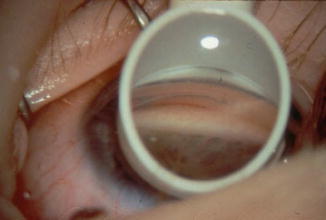
Fig. 10.2
The Hoskins-Barkan lens (Courtesy of Ocular Instruments Inc. Bellevue, Washington)
Fig. 10.3
The Swan-Jacobs lens (Courtesy of Ocular Instruments Inc. Bellevue, Washington)
Fig. 10.4
View of the pediatric angle through the Swan-Jacobs lens (Reproduced with permission from [8])
Indirect Gonioscopy
The lenses used in indirect gonioscopy use mirrors to overcome total internal reflection. The mirror redirects light from the angle so that it exits the eye perpendicularly to the lens-air interface.
The Posner lens (Fig. 10.5) has four identical mirrors. This allows examination of all four quadrants of the angle while moving the slit lamp and with only minimal rotation of the lens to look in the areas skipped by each mirror. Because the lens has a small (9 mm) area of contact with the cornea, the angle can be deepened by pushing on the lens (indentation gonioscopy). A coupling agent is not required. The Sussman lens (Fig. 10.6) is very similar to the Posner lens, except that it has no handle. There are no particular advantages or disadvantages between these lenses, and individual preference typically determines which is used.


Fig. 10.5
The Posner lens (Courtesy of Ocular Instruments Inc. Bellevue, Washington)
Fig. 10.6
The Sussman lens (Courtesy of Ocular Instruments Inc. Bellevue, Washington)
The Goldmann three-mirror lens (Fig. 10.7a, b) has one mirror dedicated to viewing the angle. There are two additional mirrors for examination of the peripheral retina. The Goldmann lens is coupled to the cornea by means of a viscous methylcellulose fluid. The lens has a broad (12 mm) area of contact with the globe and can, under the application of pressure, artificially close the angle. It cannot be used to perform indentation gonioscopy, but provides an outstanding view of the angle. A single-mirror Goldmann lens has only the gonioscopic mirror.
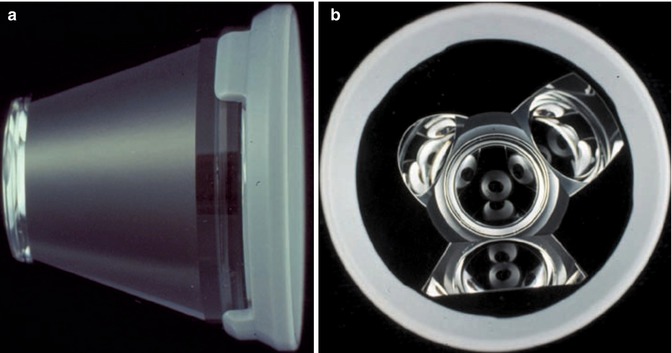
Fig. 10.7
The Goldmann three-mirror lens. (a) Outside view. (b) Inside view (Courtesy of Haag-Streit, Koeniz, Switzerland)
Comparison of Direct and Indirect Gonioscopy
Both direct and indirect gonioscopy have advantages and disadvantages.
Although direct gonioscopy is no longer widely practiced outside the operating room, it does have certain advantages over indirect gonioscopy. Direct gonioscopy provides a straight-on view of the angle rather than the mirror image given by the indirect lenses. As a result, it is much easier to avoid becoming disoriented when documenting localization of findings. Direct gonioscopy permits the examiner to vary the angle of visualization more easily. Therefore, the examiner can look into a narrow angle to see if it is a steep approach to an open angle or a completely closed angle.
The major disadvantage of direct gonioscopy is its inconvenience. The patient has to lie supine, which is not compatible with the standard layout and patient scheduling in most outpatient eye clinics.
Indirect lenses have several advantages that have made them the preferred lenses for most ophthalmologists. The first advantage, specific to the four-mirror lenses, is that they do not require viscous coupling agents, which can alter the view of the fundus and diminish photographic quality. Because only a topical anesthetic is required, one can perform applanation tonometry and then move directly to gonioscopic exam. The slit lamp serves as a source of variable magnification and illumination. The slit beam can create a corneal wedge to help to define the structures of the angle. Indentation gonioscopy can be performed with the Posner or Sussman lens to distinguish appositional from synechial angle closure, allowing for a much more dynamic exam.
Indirect lenses have the disadvantage of giving a mirror-image view of the angle, which can be somewhat confusing until the technique has been practiced. This becomes relevant when trying to localize an angle mass or an area of synechiae or angle recession. It is also easy to open or close the angle inadvertently by applying excessive pressure to the indirect lenses. These lenses may exaggerate the degree of angle narrowing and are less able to provide a view into the depths of a narrow angle [2]. This is also more common for beginners and becomes less problematic with experience.
Gonioscopy General Guidelines
The eye should be examined carefully with the slit lamp before beginning gonioscopy. Many clues exist on slit lamp exam to predict possible findings on the gonioscopic exam, such as corneal endothelial pigment, iris transillumination defects, or posterior embryotoxon. An estimation of chamber depth can be obtained at the slit lamp although an apparently deep chamber should not exclude the need for gonioscopy. Tonometry should be performed prior to gonioscopy as pressure on the eye from the examining lens can temporarily lower the intraocular pressure.
The eye should be anesthetized with a topical agent. The patient must be comfortably positioned at the slit lamp. Align the lateral canthus of the patient’s eye with the canthal marker of the slit lamp. It is inconvenient to have the patient’s head too high or too low and have to pause the examination in order to reposition. The lens can then be gently placed on the surface of the eye (Fig. 10.8). If the patient is properly aligned, one can see all quadrants of the angle, only pausing to move the lens from one eye to the other. The examiner should try to brace his or her elbow on either the slit lamp table or an additional support. Often times a lens case will suffice (Fig. 10.9). Slit lamp magnification should start at low power as is typical for a standard slit lamp or fundus exam. Bright illumination can be employed to identify the key landmarks, and then the beam length should be decreased and narrowed in order to grade the angle. When the angle depth is being graded, light should not be allowed to enter the pupil as pupillary constriction will place the iris on stretch and may the angle appear more open than it is in dark conditions.




