Chapter 20
GLAUCOMA

Ocular trauma is an important, usually preventable cause of glaucoma. Injury is an especially common etiology for elevated IOP in young patients. In one study, trauma was the cause of glaucoma in 36% of patients under the age of 30, whereas it was the etiology in only 1.3% of patients over 30 years of age.1
PITFALL
One reason why glaucoma is an important cause of trauma-related vision loss is that it frequently occurs late, after other problems have been treated or stabilized. Given its insidious nature, it is unsuspected by the physician or by the patient; opportunities to prevent permanent visual loss due to elevated IOP may have been missed.
In discussing trauma-associated glaucoma, it is useful to categorize the type of injury as open globe or closed globe because both the mechanisms and the management are unique.a It is also helpful to distinguish between glaucoma that develops immediately following trauma and that with a delayed onset2 (Table 20–1). Finally, high IOP may result from non-mechanical factors.
GLAUCOMA ASSOCIATED WITH CLOSED GLOBE TRAUMA
Epidemiology Contusion is responsible for a large percentage of ocular trauma. Data derived from hospital discharge summaries in the United States between 1984 to 1987 revealed an annual ocular trauma rate of 13.2 per 100,000 population; 40% of these were coded as contusion of the eyeball, adnexa, or orbit.3
Pathophysiology As an object strikes the eye, the force can result in ocular damage from two mechanisms:
• direct transfer of energy: impact by a blunt agent leads to the transference of force vectors radiating from the point of contact. If the force is significant, it can lead to necrosis of the tissue; and
• secondary changes in ocular shape: as the globe is compressed in the anterior-posterior direction, it elongates equatorially (Fig. 20–1). The central lens-iris diaphragm is forced posteriorly while at the same time the attachments of these structures are anchored to the eyewall, which is moving in a perpendicular direction. This leads to shearing forces that can tear these structures at their root.
PEARL… Acutely following contusion injury, some eyes have a temporary reduction in their IOP. This is thought to result from decreased aqueous production and possibly from increased outflow.
| Closed globe, earlier onset | traumatic uveitis | ||||
| trabecular meshwork disruption | |||||
| hemorrhage-associated | |||||
| lens-associated | |||||
| Closed globe, later onset | angle recession | ||||
| closure of cyclodialysis cleft | |||||
| hemorrhage-associated | ghost cell | ||||
| hemolytic | |||||
| hemosiderotic | |||||
| lens-associated | subluxation | ||||
| phacomorphic | |||||
| particle | |||||
| uveitis | |||||
| Open globe; | inflammation | ||||
| flat AC | |||||
| epithelial downgrowth | |||||
| intraocular hemorrhage | ghost cell | ||||
| hemolytic | |||||
| hemosiderotic | |||||
| IOFB | |||||
| Chemical | |||||
| Thermal | |||||
| Electrical |
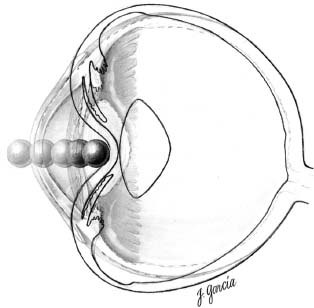
FIGURE 20–1 When a blunt object strikes the eye, it causes ocular shortening in the anteroposterior dimension and elongation of the globe equatorially. As this occurs, the lens-iris diaphragm is pushed posteriorly in its central aspect while the peripheral aspects of these structures are expanding with the equator of the globe. This leads to tearing of the structures in the anterior segment, particularly in the angle.
Early-Onset Glaucomas
Trabecular Meshwork Obstruction/Inflammation
Inflammatory cells obstruct the (inflammed) trabecular meshwork, decreasing outflow facility. This IOP elevation may be seen even without:
• hyphema;
• angle recession; or
• disruption of the trabecular meshwork.
Treatment requires:
• close monitoring, as most cases are self-limited; and
• topical corticosteroids (typically necessary only for a short period).
Trabecular Disruption
Trauma-related changes in the trabecular meshwork have been documented with gonioscopy within 48 hours of injury.4 Findings include:
• sharply demarcated hemorrhage into Schlemm’s canal;
• full-thickness rupture of the trabecular meshwork; and, occasionally,
• a trabecular flap, hinged at the region of the scleral spur; or
• cyclodialysis (see also Chapter 19).b
Hyphema
It commonly results from contusion, which causes a tear in the ciliary body and bleeding from the small branches of the major arterial circle of the iris. Less commonly, bleeding may result from tears within the iris or trabecular meshwork.
Hyphema is an indicator of significant trauma and may lead to IOP elevation by several mechanisms:
• disruption of the trabecular meshwork;
• obstruction of the meshwork with RBCs; or
• obstruction of the meshwork with inflammatory cells and fibrin.
Treatment If conservative management does not reduce the IOP, surgical intervention may be necessary (see Chapter 17).
Delayed-Onset Glaucomas
Angle Recession
PEARL… The term “angle recession glaucoma” is somewhat misleading, as the recessed angle, caused by contusion,6 is not the cause of the glaucoma, but rather an indicator of significant trauma to the eye.7
Epidemiology Angle recession is a common consequence of contusion. Among patients with a hyphema, angle recession has been observed in 71 to 100% of eyes.8–11
Some authors have sought to correlate the amount of angle recession with the risk of glaucoma development. An increased risk of glaucoma development was found if the angle recession exceeded 1801 or 2404 degrees.
It must be understood, however, that patients who develop glaucoma following trauma may have an underlying predisposition to reduced aqueous flow:
• these patients frequently have IOP elevation in the fellow eye14–16; and
• elderly patients more frequently develop postcontusion glaucoma.17
Pathophysiology (Fig. 20–2) includes the following.
• Angle recession represents a tear between the longitudinal and circular fibers of the ciliary body.
• Acutely, iridodialysis (a tear of the peripheral iris attachment), which separates the iris from the ciliary body, may be also be present (see Chapter 18).
• Cyclodialysis (a separation of the ciliary body attachment to the scleral spur), may also be seen.
• Elevated IOP results not from the angle recession but from collateral damage and scarring of the trabecular meshwork. Following trauma, there are tears in the trabecular meshwork posterior to Schwalbe’s line; this produces a flap of trabecular tissue that was hinged at the scleral spur. Scarring ensues and leads to chronic obstruction.15
• An additional mechanism for IOP elevation is the extension of an endothelial layer with a Descemet-like membrane from the cornea over the AC.7,18,19,c
Clinical Picture Patients may present during the first year after injury or as late as more than 10 years after the trauma.15 Typically, patients present several years following the injury.
The amount of angle recession affects the time of presentation. Patients with more than 270 degrees of recession usually present earlier.15
Evaluation In patients with unilateral glaucoma, a careful history of the trauma must be obtained.
The slit-lamp/IBO examination may reveal:
• discrepancy of AC depth;
• difference in pigmentation between the two irises and in the angle;
• tears in the iris root or sphincter;
• increased peripheral anterior synechiae in the area of trauma;
• paralysis of the pupillary sphincter20;
• Vossius ring or circular pattern of pigment deposition on the lens;
• zonular rupture with prolapse of vitreous into the AC (Fig. 20–3);
• iridodonesis and phacodonesis;
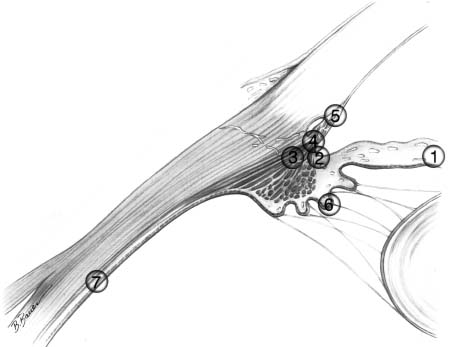
FIGURE 20–2 Seven commonly injured intraocular structures following contusion injury. 1, Iris sphincter. 2, Iris root (iridodialysis). 3, Between the longitudinal and circular muscles of the ciliary body (angle recession). 4, At the insertion of the ciliary body (cyclodialysis). 5, In the trabecular meshwork. 6, Lens zonules (subluxation or dislocation of lens). 7, Retinal tears or dialysis. (From Pieramici D, Parver LM. A mechanistic approach to ocular trauma. Ophthalmol Clin North Am. 1995;8:575. Reprinted by permission from WB Saunders.)

FIGURE 20–3 This patient experienced severe contusion to the phakic right eye a few years following radial keratotomy. Although the corneal incisions remained intact, bloody vitreous was seen in the AC, suggesting zonular dialysis.
• posterior signs of trauma (e.g., pigment in the vitreous, RPE hyperplasia, choroidal or retinal scars).
Common gonioscopic findings include:
• widened ciliary body;
• prominent scleral spur secondary to angle recession; and
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


