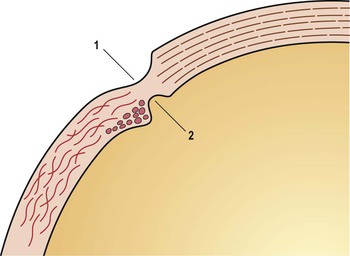
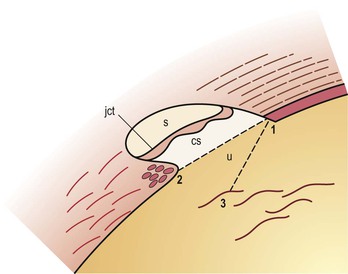
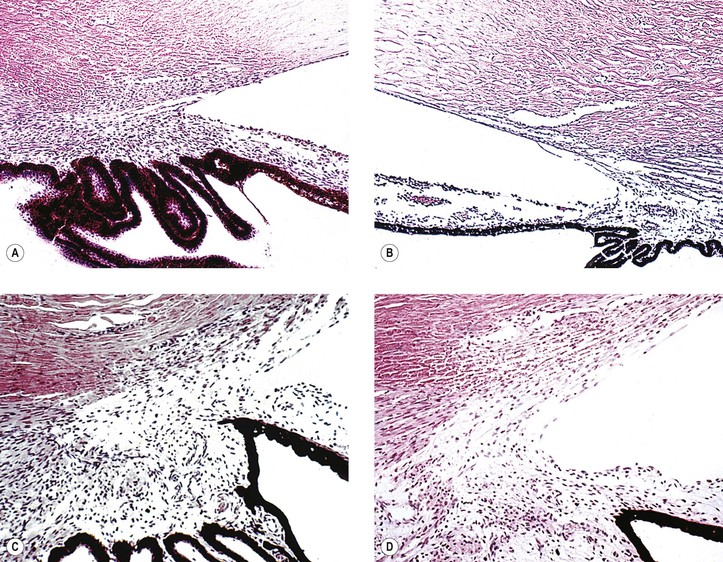
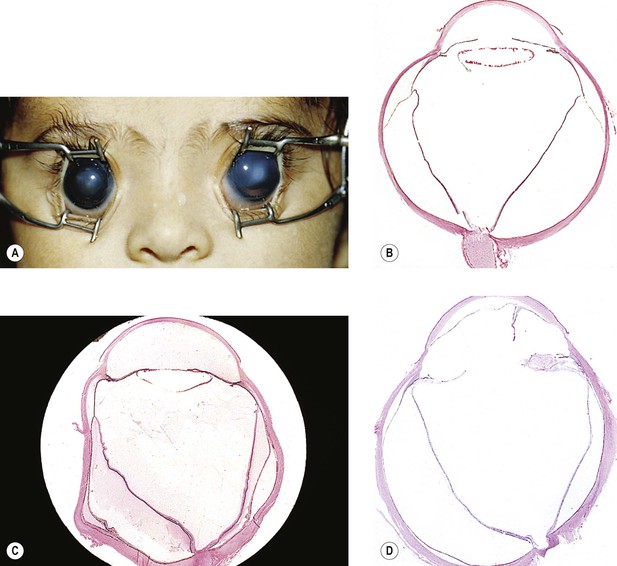
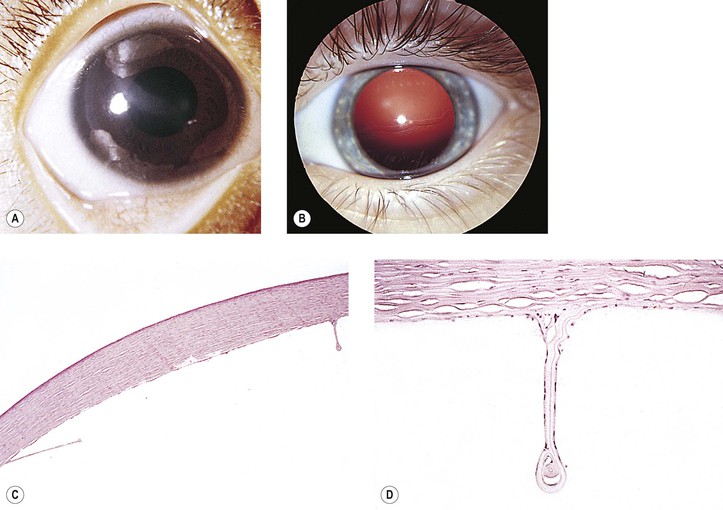
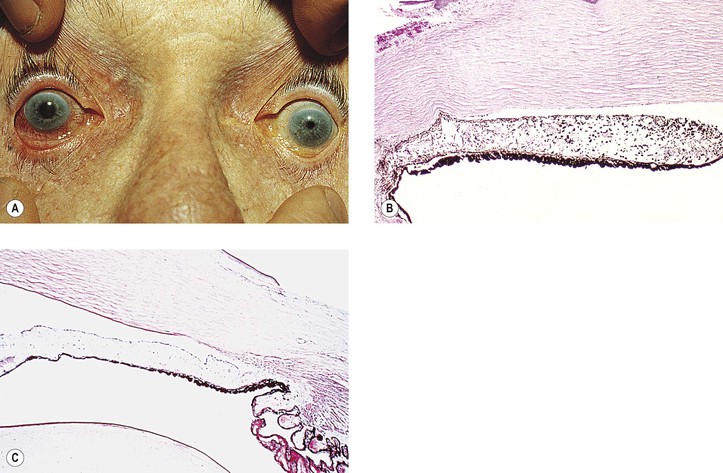
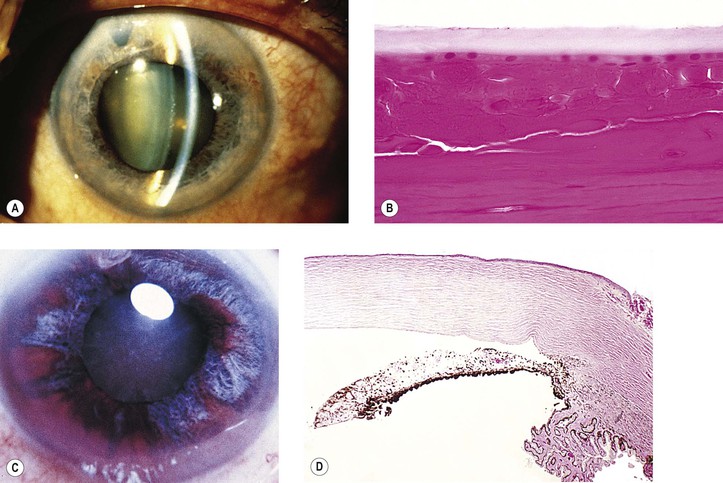
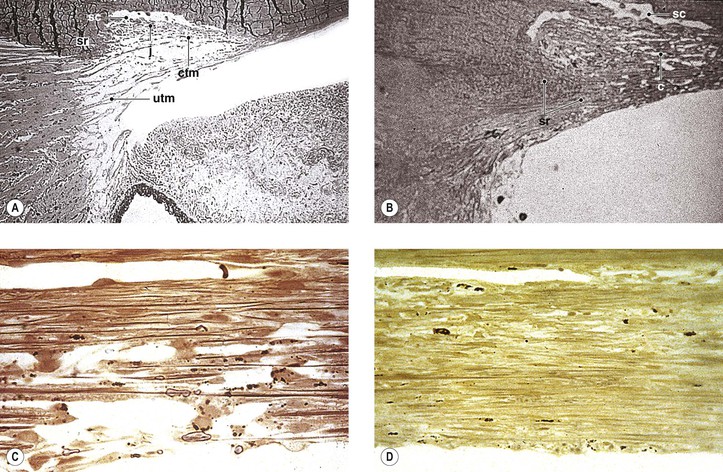
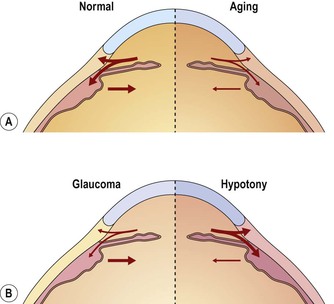
I. The outermost or corneoscleral layer of the eye can be separated into corneal and scleral portions by two circumferential grooves—a shallow outer one, the outer scleral sulcus, and a deeper inner one, the inner scleral sulcus. C. Deep within this inner sulcus and applied closely to the collagenous tissue of the corneosclera lies the large vessel called the canal of Schlemm. 3. The inner wall rests on a thinner or patchy basement membrane that is associated with a zone of delicate connective tissue, the juxtacanalicular connective tissue. 4. Pores are present in the wall of Schlemm’s canal. B. The meshwork may be easily and usefully separated into two parts by an imaginary line extending from the scleral roll to the end of Descemet’s membrane (see Fig. 16.2). The cell and molecular biology and gene rearrangement aspects of the glaucomas are fascinating, but an in-depth analysis of these matters is beyond the scope of our discussion. For example, genome-wide expression profiling of patients with primary open-angle glaucoma (POAG) identified 563 genes that were significantly dysregulated in POAG compared with normal controls. These genes impacted numerous functions, including nucleoside, nucleotide, and nucleic acid metabolism; the mitogen-activated protein kinase kinase kinase (MAPKKK) cascade; apoptosis; protein synthesis; cell cycle; intracellular signaling cascade; and nervous system development and function. Therefore, we highlight only a few salient facts regarding these areas. Currently, 15 chromosome loci, which are designated GLC1A to GLC10, are associated with POAG. Candidate genes include myocilin (GLC1A), WD40-repeat36 (GLC1G), optineurin (GLC1E), and neurotrophin-4 (NTF-4) (optineurin is discussed with normal pressure glaucoma later in this chapter). Nevertheless, it has been estimated that mutations in known glaucoma genes account for less than 15% of cases. The prevalence of heterozygous cytochrome p450 1B1 (CY1B1) gene changes in a mixed glaucoma population suggests that the pathogenesis of glaucoma is genetically heterogeneous and may be polygenic. Single nucleotide polymorphisms (SNPs) between the CAV1 and CAV2 genes on chromosome 7q31 code for two members of the caveolin family of proteins are associated with POAG in white Americans, particularly women. These proteins impact modulation of endothelial cell membranes, which could alter the process of ocular aqueous fluid drainage. In general, however, SNPs are not discussed in any detail, but they have been described elsewhere (see Bibliography). Gene copy number variations also may play a role in the development of POAG. For example, homozygous deletions that reduce galactosylceramidase activity may increase the risk of POAG. I. Glaucoma is characterized by an intraocular pressure (IOP) sufficient to produce ocular tissue damage, either transient or permanent. A. Glaucoma is a “family” of diseases having in common a type of optic atrophy called optic nerve head cupping or excavation. B. Although most individuals associate glaucoma with an elevated IOP, the pressure may, in fact, be within the statistically “normal” range and still cause ocular tissue damage in normal-tension (improperly called low-tension) glaucoma. 1. IOP is a risk factor for glaucoma, and the higher the pressure, the greater the probability of the development of the disorder. a. The accurate measurement of IOP is vital to the proper diagnosis and treatment of glaucoma. c. CCT is increased in children with ocular hypertension. 2. Normal-tension glaucoma probably accounts for approximately one-third of all cases of POAG. Optineurin II. Glaucoma suspect B. POAG accounts for approximately two-thirds of all glaucoma seen in white patients. A. The rate of congenital glaucoma is from 1 : 5000 to 1 : 10,000 live births. C. Approximately 60–70% of affected children are boys. D. The disease is bilateral in 64–88% of cases. II. Pathogenesis (many theories) C. An “embryonic” anterior chamber angle that results from faulty cleavage of tissue during embryonic development of the eye prevents the aqueous from leaving the anterior chamber. 1. Histologically, the angle shows an anterior “insertion” of the iris root, anteriorly displaced ciliary processes, insertion of the ciliary meridional muscles into the trabecular meshwork instead of into (or over) the scleral roll, and mesenchymal tissue in the anterior chamber angle (Fig. 16.4). 2. Many nonglaucomatous infant eyes show a similar anterior chamber angle structure. 3. To interpret angle histology accurately, it is necessary to study truly meridional sections through the anterior chamber angle. a. Tangential sectioning makes interpretation difficult (see Figs. 16.4C and 16.4D). D. The actual cause or causes of congenital glaucoma probably remain unknown. III. Associated diseases and conditions A. Iris anomalies (see Chapter 9) 1. Hypoplasia of the iris (“aniridia”) and iris coloboma may be associated with congenital glaucoma. a. The PAX6 point mutation defect (1630A > T) on band p13 of chromosome 11 has been associated with some cases of aniridia. PAX6 mutations result in alterations in corneal cytokeratin expression, cell adhesion, and glycoconjugate expression. There is also corneal stem cell deficiency, which contributes to associated keratopathy. B. Axenfeld’s anomaly and Rieger’s syndrome (see Chapter 8) C. Peters’ anomaly (see Chapters 2 and 8). Peters’ anomaly and primary congenital glaucoma may share a common molecular pathophysiology. Both of these disorders can be associated with mutation in the cytochrome P4501B1 (CYP1B1) gene (discussed previously). D. Phakomatoses 1. Sturge–Weber syndrome (see Chapter 2) 2. Neurofibromatosis (see Chapter 2) E. Lowe’s syndrome (see Chapter 10) H. Marfan’s syndrome (see Chapter 10) I. Homocystinuria (see Chapter 10) J. Microcornea (see Chapter 8) K. Spherophakia (see Chapter 10) L. Chromosomal abnormalities (e.g., trisomy 13; see Chapter 2) M. Persistent hyperplastic primary vitreous (see Chapter 18) N. Retinopathy of prematurity (see Chapter 18) O. Retinoblastoma (see Chapter 18) P. Juvenile xanthogranuloma (see Chapter 9) V. Neurofibromatosis type 1 should be excluded in newborns with unilateral congenital glaucoma. IV. Secondary histologic ocular effects in young eyes (<10 years of age) A. Buphthalmos (“large eye”) is caused by an enlargement, stretching, and thinning of the coats of the eye, especially marked in the anterior segment, resulting in a deep anterior chamber (Fig. 16.5). Subluxated lenses may develop in these enlarged eyes. B. Ruptures of Descemet’s membrane (Haab’s striae) may be found in the enlarged corneas (Fig. 16.6), are usually horizontal in the central cornea but concentric toward the limbus, are located mainly in the lower half, and are often associated with corneal edema. C. The limbal region becomes stretched and thin, with a resultant limbal ectasia (see Fig. 16.5). E. Continued high IOP may cause atrophy of the ciliary body, choroid, and retina; cupping of the optic disc (see Fig. 16.5); and atrophy of the optic nerve. II. Optical coherence tomography and ultrasound biomicroscopy can be utilized to evaluate the anatomic configuration of the anterior chamber angle and adjacent structures for the classification of the pathophysiology of the glaucomas. A. Specific features with such imaging studies that may contribute to angle-closure include: 3. Smaller anterior chamber width, area, and volume 4. Dynamic increase or lesser reduction in iris volume during dilation 5. Choroidal expansion accompanying angle-closure III. Closed-angle (narrow-angle; angle-closure; acute congestive) glaucoma (Figs. 16.7 and 16.8) A. In anatomically predisposed eyes, primary closed-angle glaucoma develops. 2. Small, hypermetropic eyes are especially vulnerable to angle-closure. 3. The lens is normal-sized or large. C. A sudden rise in IOP results from the peripheral iris being in apposition to the filtering trabecular meshwork from the pupillary block mechanisms except in the plateau iris syndrome, which in its pure form does not involve pupillary block. F. Histology b. Segmental iris atrophy is usually seen in the upper half of the iris in a sector configuration. 2. Irregular pupil results from necrosis of the dilator and sphincter muscles. a. Histologically, segments of the dilator muscle or its entire length are absent. b. The sphincter muscle shows varying degrees of atrophy. 3. Glaukomflecken (cataracta disseminata subcapsularis glaukomatosa; see Fig. 16.8) a. Glaukomflecken probably results from interference with the normal metabolism of the anterior lens cells due to a stagnation of aqueous humor that contains toxic products of necrosis or from foci of pressure necrosis (see Chapter 10). b. Anterior subcapsular, multiple, tiny gray-white lenticular opacities are seen. b. Irreversible vision impairment after an acute attack is mainly caused by optic nerve damage. G. Failure to reverse the initial attack of angle closure can result in chronic angle-closure glaucoma. 1. This entity can be confused clinically with chronic open-angle glaucoma unless careful gonioscopy is performed routinely on all suspected cases of glaucoma. 2. Histology IV. Chronic open-angle (chronic simple) glaucoma (POAG) (Figs. 16.9 and 16.10) A. The angle appears normal gonioscopically. C. The condition is most often bilateral. 1. Glaucoma may develop in one eye months to years before the fellow eye. 2. One eye may be more severely affected than the other eye. D. Prevalence (see section Introduction) 1. In most cases, the condition is probably inherited as an autosomal-recessive trait. 2. Myocilin F. Normal-tension (improperly called low-tension) glaucoma is a subdivision of POAG (see section Introduction in this chapter). G. Histology and pathophysiology 1. Optic nerve (see later in this chapter) 2. Little is known about the early histologic changes that take place in the region of the drainage angle because the number of human eyes that have well-characterized early open-angle glaucoma available for histologic examination is small (see Fig. 16.9). 4. Aging changes in the drainage angle of the anterior chamber d. The degree of obstruction is a quantitative problem; two extremes of excessive obstruction are: e. The two major aging changes—each may be seen in almost pure form, or they may be combined. 1) They may also be associated with proliferations of trabecular endothelial cells in the meshwork. 2) COAG depends on the amount of aqueous inflow and the degree of obstruction to outflow caused by the aging changes (see Fig. 16.10). f. Other changes in the trabecular meshwork in POAG include loss of cells, increased accumulation of extracellular matrix, changes in cytoskeleton, cellular senescence, and the process of subclinical inflammation. Oxidative stress is likely to be one important mechanism in the pathogenesis of POAG. I. Chronic primary angle-closure glaucoma B. Histologically, peripheral anterior synechiae are seen, sometimes broad based. II. Phacomorphic V. Iridocorneal endothelial (ICE) syndrome 1. All three entities share a basic corneal endothelial defect and iris involvement. 3. Glaucoma occurs in approximately 50% of cases. 5. Each variant is described separately, but all are considered to belong to the ICE syndrome. Posterior polymorphous dystrophy (PPMD; see Chapter 8) shares some characteristics with the ICE syndrome (Table 16.1
Glaucoma
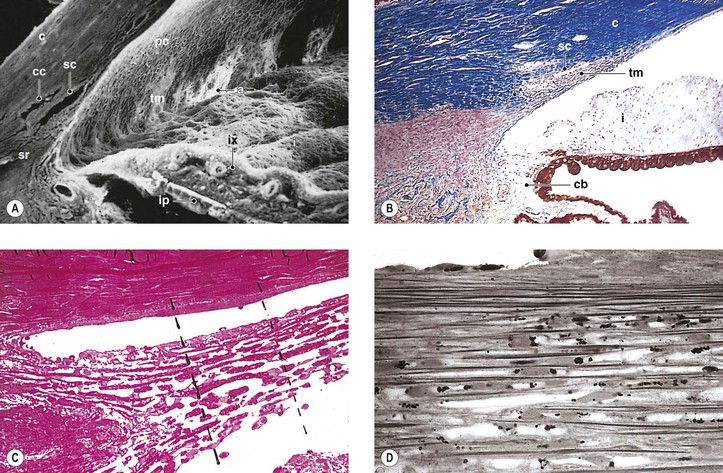
Normal Anatomy (Figs. 16.1–16.3)
Introduction
Currently, 15 gene loci, designated GLC1A to GLC10, are associated with POAG. The optinuerin gene is associated with several disorders, including glaucoma, amyotrophic lateral sclerosis, other neurodegenerative disorders, and Paget’s disease of bone. A glaucoma-causing gene has been identified at GLC1E, and sequence variations in this optineurin (OPTN) gene on GLC1E have been found to be associated with the development of normal-tension glaucoma. The gene is located on chromosome 10. The glaucoma associated with optineurin is not characterized by marked IOP elevation. Rather, the E50K mutation in the optineurin gene is associated with increased severity of normal-tension glaucoma in white and Latino populations. There may be racial differences in glaucoma-associated optineurin genotypes. Its primary effect may be to increase susceptibility of retinal ganglion cells to premature cell death. Thus, optineurin may serve an optic nerve protective effect that is lost through mutation. Optineurin gene alterations do not appear to have a significant role in typical POAG.
Impaired Outflow
Congenital Glaucoma
Primary Glaucoma (Closed- and Open-Angle)
A founder gene effect is probably related to two families of the Faroe Islands with hereditary high hyperopia, angle-closure glaucoma, uveal effusion, cataract, esotropia, and amblyopia.
The association of typical acute closed-angle glaucoma with increasing age is due, in part, to progressive pupillary block from the increase in lens size as it adds layers of lens fibers over time.
Chronic angle-closure glaucoma is associated with the necessity of continued treatment and subsequent procedures even in the presence of a patent iridotomy.
There is disorganization of the trabecular architecture, narrowing or loss of trabecular spaces, scarring of the trabecular beams, trabecular endothelial cell loss, deposition of banded fibrillar material, and melanin pigment deposition.
Myocilin was the first gene to be associated with glaucoma. Myocilin is the most frequently mutated gene in POAG patients worldwide. There are myocilin genotype–phenotype correlations, such as age of diagnosis, maximum IOP, and response to medical therapy. Mutations in the myocilin gene are present in 1–4% of POAG patients but not in patients with pseudoexfoliation. Myocilin gene is located on chromosome 1, localized to the olfactomedin domain, and was the first gene identified for POAG in the GLC1A locus. Its associated glaucoma is transmitted as an autosomal-dominant trait. There appears to be compromised stability of the protein, which categorizes the resulting disorder as a disease of protein misfolding. There is strong evidence that myocilin polymorphisms are related to POAG susceptibility with significant racial variation such that for whites Q368x is most important, whereas T353I is not important for Asians. The Gln48His mutation is unique to Indian patients. There is a low prevalence of myocilin mutations in African-Americans with POAG.
Secondary Closed-Angle Glaucoma
Causes
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree