Purpose
To describe the features of an artifact on near-infrared reflectance and MultiColor imaging, termed “ghost maculopathy,” and to illustrate how it may masquerade as true chorioretinal pathology.
Design
This was a retrospective, observational case series.
Methods
The authors studied 144 eyes of 72 consecutive patients in a vitreoretinal clinical practice, reviewing multimodal imaging including color and red-free fundus photography, fundus autofluorescence (FAF), near-infrared reflectance, MultiColor imaging, and spectral-domain optical coherence tomography (SD OCT).
Results
In 36 of 144 eyes (25%), there was an appearance of a hyper-reflective spot on near-infrared reflectance and MultiColor imaging, located at the macula, nasal or superonasal to the fovea, which did not correspond to any apparent lesion on color and red-free fundus photography, FAF, or SD OCT. This spot was termed the “ghost image” in this phenomenon of “ghost maculopathy.” The ghost image was present consistently on near-infrared reflectance and MultiColor imaging in all 36 eyes at every imaging encounter, showing minimal and subtle variability in its shape and location within each eye; however, it showed large interindividual variability in size, shape, location, and reflectivity between different eyes. Nine eyes were found to have a similar hyper-reflective spot resembling that in ghost maculopathy, but corresponding SD OCT images were consistent with diagnoses of choroidal nevus, age-related macular degeneration, and multifocal choroiditis. All eyes with ghost maculopathy were found to be pseudophakic with a posterior chamber intraocular lens.
Conclusion
Ghost maculopathy is the phenomenon of an imaging artifact appearing at the macula on near-infrared reflectance and MultiColor imaging that occurs predominantly in pseudophakic patients and may be mistaken for true chorioretinal pathology. Awareness of this artifact is prudent to avoid misinterpretation of clinical findings and possible unnecessary over-investigation.
Near-infrared light is well suited for use in imaging the subretinal structures, as it largely avoids absorption and reflection by the layers of the neuroretina and penetrates readily to the level of the retinal pigment epithelium (RPE) and choroid. Dallow first suggested the use of near-infrared in 1974 but gained little support at the time. In 1996, Elsner and associates demonstrated near-infrared visibility of subretinal structures in macular degeneration using a confocal scanning laser ophthalmolscope (SLO). Subsequently, this technique has been extended to polarization-sensitive near-infrared and, only recently, near-infrared reflectance imaging has been used to capture the appearance of choroidal neovascularization (CNV) in age-related macular degeneration (AMD).
The Heidelberg Spectralis (Heidelberg Engineering, Heidelberg, Germany), uses confocal SLO to achieve high-contrast near-infrared reflectance images and applies an 830 nm laser source to acquire high-reflectance images in the near-infrared. More recently, Heidelberg Engineering has introduced MultiColor scanning laser imaging that uses multiple laser colors (infrared [820 nm], green [515 nm], and blue [488 nm]) simultaneously to selectively capture and display information originating from different retinal structures. Blue reflectance produces detailed images of epiretinal membranes, retinal nerve fiber layer thinning, and macular pigment changes. Green laser provides detailed views of retinal vasculature and intraretinal lipid exudation, while infrared is useful for identifying drusen and RPE.
It is well known that with near-infrared reflectance and MultiColor imaging, the normal foveal umbo can appear as a hyper-reflective spot; however, the appearance of other hyper-reflective imaging artifacts has not been described previously. As experience with these imaging techniques is relatively new, interpretation of acquired images still involves close examination and clinician experience. This study aims to highlight an artifact, unrelated to the foveal umbo, that can occur with these imaging techniques and may masquerade as true chorioretinal pathology.
Methods
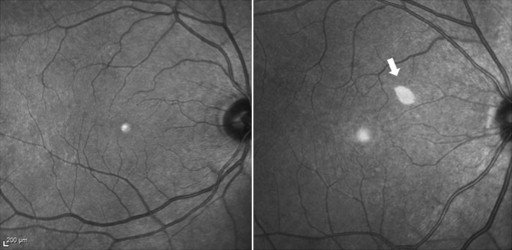
This was a retrospective, observational case series of 72 consecutive patients seen by a single physician (K.B.F.) in a vitreoretinal referral practice located in New York, New York, USA on 2 typical full-day consultation clinic sessions. Patients with the appearance of a hyper-reflective spot at the macula on near-infrared reflectance that was differentiated from the normal hyper-reflectivity seen at the foveal umbo were identified ( Figure 1 ). This spot was termed the “ghost image” in this phenomenon of “ghost maculopathy.” Medical records and multimodal images including color and red-free fundus photography, fundus autofluorescence (FAF), near-infrared reflectance, MultiColor scanning laser imaging, and spectral-domain optical coherence tomography (SD OCT) were reviewed. FAF, near-infrared reflectance, MultiColor imaging, and SD OCT were obtained with the Heidelberg Spectralis (Heidelberg Engineering, Heidelberg, Germany). Color and red-free fundus photographs were obtained with the Topcon TRC-50IX (Topcon Corporation, Tokyo, Japan) fundus camera. All images of retrospective clinic visits up to 4 years of retrospective follow-up were reviewed. This study had Western Institutional Review Board approval and was compliant with the Health Insurance Portability and Accountability Act.
Results
In 36 of 144 eyes (25%), there was the appearance of a hyper-reflective spot on near-infrared reflectance and MultiColor imaging, located at the macula, that did not correspond to any apparent lesion on color and red-free fundus photography, FAF, or SD OCT and was therefore given the term “ghost maculopathy.” The mean age of the 36 patients with ghost maculopathy was 83 years (52–100 years), 8 (22%) were male and 28 (78%) were female. All eyes with ghost maculopathy were found to have the presence of a posterior chamber intraocular lens (PC-IOL) implanted at the time of cataract surgery. Among the 75 pseudophakic eyes, the prevalence of ghost maculopathy was 48% (75/144). Of note, ghost maculopathy was not seen in any of the 69 phakic eyes.
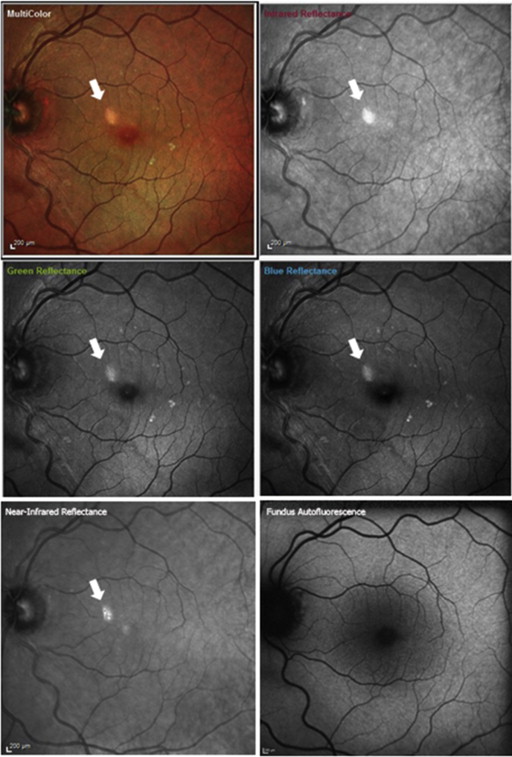
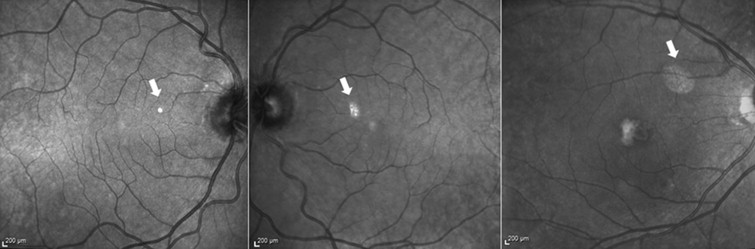
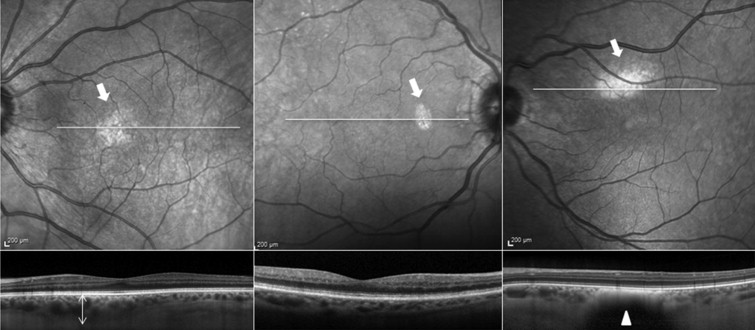
The ghost image was present consistently on near-infrared reflectance and MultiColor imaging in all 36 eyes at every imaging encounter but never in FAF or SD OCT ( Figure 2 ). Ghost maculopathy showed large interindividual variability in size, shape, location, and reflectivity between different eyes. Its appearance ranged from a small, well-circumscribed, circular or oval or crescent-shaped spot to a larger, more diffuse reflectance with indistinct borders. Its location could vary, although it was usually nasal or superonasal to the fovea. The ghost image always appeared as hyper-reflective, although its reflectance could vary from solid, bright white to a granular or speckled, less intense white ( Figure 3 ).
Ghost maculopathy showed minimal and subtle variability in its shape and location within each eye at every clinic encounter of up to 4 years of follow-up visits ( Figure 4 ). In 2 patients who had cataract surgery within the course of their follow-up, the appearance of the ghost image was observed to occur only after the implantation of the intraocular lens.

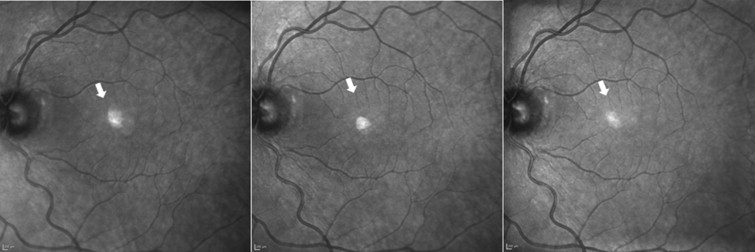
In an attempt to eliminate the artifact, repeated near-infrared reflectance images at a single setting with varying angles of incident light were obtained. This resulted in subtle shifts in the location of the lesion ( Figure 5 ). The ghost image could not be completely eliminated without compromising the image quality or resulting in a complete blackened-out fundus image where no details of the fundus were visible.
In 9 eyes, we observed the appearance of a similar hyper-reflective spot resembling the ghost image. However, these spots corresponded to true pathology seen on SD OCT images and their diagnoses included choroidal nevus, AMD, and multifocal choroiditis ( Figures 6, 7 and 8 ).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


