4 General Otolaryngology
Statistics
1 | Define sensitivity. ( | The ability of the test to identify correctly those patients with the disease |
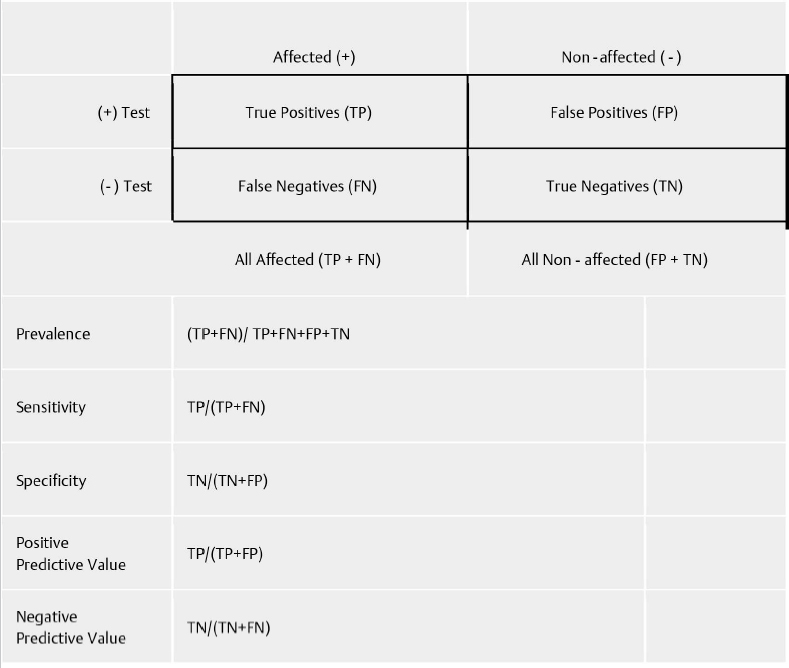
Fig. 4.1 Biostatistics calculations.
2 | Define specificity. | The ability of the test to identify correctly those patients without the disease |
3 | Is high sensitivity or high specificity most important for a screening test? | Sensitivity |
4 | Define a type 1 error. | The chance of testing positive among those without the condition; false-positive rate = 1 specificity. |
5 | Define a type 2 error. | The chance of testing negative among those with the condition; false negative rate = 1-sensitivity. |
Define positive predictive value. | The chance of having the condition among those that test positive | |
7 | Define negative predictive value. The chance of not having the condition among those that test negative | Imaging |
8 | A cervical spine X-ray revealing a greater than 5-mm widening of the predentate space (between the anterior surface of the dens and the posterior surface of the C1 tubercle) is worrisome for what traumatic injury? | Atlantoaxial dissociation |
9 | Conventional radiography of the facial bones and neck has been largely replaced by computed tomography (CT). What traditional views were used to view the following: • Frontal, maxillary, and sphenoid sinus • Frontal sinuses, posterior ethmoid air cells, orbital floors • Maxillary sinuses, anterior ethmoid air cells, orbital floors • Sphenoid sinuses, anterior and posterior walls of the frontal sinuses • Soft tissue of the neck | • Lateral view (5 degrees off true lateral) • Caldwell view (15 degrees off caudal angulation) • Waters view (neck in 33 degrees of extension) • Submentovertex view (anteroposterior [AP] projection, head in 90 degrees of extension) • AP and lateral views |
10 | In a stable pediatric patient with stridor, what radiography is appropriate? | AP and lateral neck films to evaluate for retropharyngeal abscess, croup, epiglottitis, and radiopaque foreign body |
11 | What are the most common findings on chest radiography in a patient with a witnessed foreign-body aspiration and clinical signs suggestive of aspiration? | Mediastinal shift, unilateral hyperinflation, atelectasis, and a foreign object if radiopaque |
12 | Although they have been largely replaced by CT scan, radiographs of the temporal bone are occasionally necessary. Name the following views: • Lateral view of the mastoid with 30 degrees of cephalocaudad angulation • View of the petrous apex with patient facing the film, head slightly flexed and turned 45 degrees opposite the film • Comparison of both mastoid bones and petrous pyramids via AP view with a 30-degree tilt | • Schüller view • Stenvers view • Towne view |
13 | Why is a CT scan typically a more appropriate imaging study in evaluating patients with a potential deep neck space infection instead of magnetic resonance imaging (MRI)? | Although MRI provides better soft tissue definition, it is expensive and requires a lengthy scan time compared with CT and therefore may necessitate sedation of a child or a distressed patient and increase the likelihood of airway compromise. |
14 | On T1-weighted MRI, contrast-enhancing tumors may be hidden by surrounding fat. What technique can be used to achieve better visualization of the tumor? | Fat suppression |
15 | Describe the T1-weighted appearance of water and fat on MRI. | Low intensity and high intensity, respectively |
16 | What are some of the contraindications to MRI use? | Electromagnetic force can cause serious malfunction to cardiac pacemakers and cochlear implants (although new techniques have been developed that allow cochlear implant recipients the ability to have MRI studies). Some older vascular clips and ossicular prostheses contain paramagnetic components, and unless these are known to be MRI compatible, another modality should be used. |
What does SUV stand for in regard to positron emission tomography (PET) imaging? | Standardized uptake value, which provides a semiquantitative index of radio tracer uptake | |
18 | What does the presence of an echogenic (fatty) hilum typically indicate during ultrasound examination of the neck? | Benign disease. Normal lymph nodes have an echogenic hilum, whereas it is reported that there is an absent hilum in 96 of metastatic lymph nodes. |
19 | Can the location of normal parathyroid glands be identified on ultrasound examination of the thyroid and neck? | Normal parathyroid glands are not usually visible because of their small size and similar echo texture to adjacent thyroid tissue. |
20 | What is acoustic shadowing in ultrasound imaging? | Diminished sound or loss of sound posterior to a strongly reflecting or attenuating structure |
Pharmacology
21 | Review the differences between first-generation and second-generation antihistamines. | Compared with first-generation antihistamines, second-generation medications generally have a longer duration of action, have less central nervous system (CNS) penetration, and are less sedating. |
22 | Review contraindications to glucocorticoid steroid use. | Psychosis, severe diabetes, peptic ulcer disease, congestive heart failure, severe hypertension, systemic tuberculosis, osteoporosis |
23 | Describe the features of ototoxicity associated with salicylate use. | Reversible sensorineural hearing loss and tinnitus, hypothesized to result from disruption of oxidative phosphorylation. Its use does not produce histologic changes. |
24 | What severe neurologic side effect is associated with intramuscular administration of prochlorperazine? | Extrapyramidal side effects including focal dystonia |
25 | List the different amide and ester local anesthetics. | Amides have two “i’s,” whereas esters only have one “i” in their generic name. Examples of esters include benzocaine, cocaine, and tetracaine. Examples of amides include bupivacaine, lidocaine, and mepivacaine. Esters are more likely to cause an allergic reaction |
26 | What topical anesthetic reversibly binds to and inactivates sodium channels, thus inhibiting excitation of nerve endings and causing vasoconstriction? | Cocaine |
27 | What is the maximum dose of lidocaine hydrochloride? | 4 to 5 mg/kg, maximum total dose of 300 mg |
28 | What medication can be given to reverse the effects of local injectable epinephrine? | Local infusion of 1.5 to 5 mg of phentolamine |
29 | What is the mechanism of action for β-lactam antibiotics? | Binds to DD-transpeptidase (also called penicillin-binding protein) and inhibits the formation of peptidoglycan cross-links in the bacterial cell wall |
30 | What is the mechanism for acquiring penicillin resistance? | Enzymatic deactivation of penicillin G through β-lactamases and altered penicillin binding proteins |
31 | What is the mechanism of action of aminoglycosides? | They irreversibly bind to the 30S ribosome and freeze the 30S initiation complex. Additionally, they cause misreading of the mRNA code (bactericidal). |
32 | A mutation in which a gene may lead to increased aminoglycoside toxicity even at low doses? | Mitochondrial 12S ribosomal RNA gene |
33 | What are the earliest signs of aminoglycoside ototoxicity? | Tinnitus, high-frequency hearing loss, and dizziness |
34 | What is the mechanism of action of macrolides? | They inhibit translocation of the peptidyl tRNA from the A to the P site on the ribosome by binding to the 50S ribosomal RNA (bacteriostatic). |
What is the treatment of Clostridium difficile colitis? | IV or oral (PO) metronidazole or PO vancomycin | |
36 | What are the most common antibiotics that have been implicated in the development of C. difficile colitis? | Second- and third-generation cephalosporins, ampicillin/amoxicillin, and clindamycin |
37 | A child develops gray staining of the teeth with a prominent horizontal line across the upper and lower teeth after being prescribed an antibiotic. Which antibiotic was most likely prescribed? | Tetracycline |
38 | What is the mechanism of action of aspirin? | Irreversible acetylation of serine 529 of cyclooxygenase (COX) 1. Rapid onset of action if dose is 160 mg or greater. The effects of use last for the lifetime of the platelet, which is 7 to 10 days. |
39 | What is the mechanism of action of thienopyradines (e.g., clopidogrel bisulfate)? | Irreversible inhibition of the cysteine residue of the P2Y12 platelet receptor. Onset of action is rapid if patient is given a loading dose, and the effects last for the lifetime of the platelet (7 to 10 days). |
40 | What drug can be given to reverse the antiplatelet effects of nonsteroidal anti-inflammatory drugs (NSAIDs)? | Desmopressin acetate (DDAVP) |
41 | In the event of significant bleeding following administration of heparin, what medication should be considered? | Protamine. Give 1 mg for every 100 units of heparin, and closely monitor activated partial thromboplastin time (aPTT). |
42 | What is the mechanism of action of warfarin? | It is a vitamin K antagonist that inhibits the production of vitamin K-dependent clotting factors. |
Critical Care
43 | Describe the mechanism of malignant hyperthermia. | It is caused by a combination of a volatile inhalational anesthetic (commonly halothane) and the short-acting paralytic succinylcholine. An abnormal ryanodine receptor causes overwhelming amounts of calcium to be released from the sarcoplasmic reticulum of skeletal muscle, thereby initiating prolonged and intense muscle contraction. |
44 | What is the initial treatment for malignant hyperthermia? | Stop the anesthetic, give dantrolene (which prevents the release of calcium from endoplasmic reticulum), increase oxygen, and initiate cooling measures including ice packs. |
45 | What are the physical examination findings of cardiac tamponade? | Tachycardia, paradoxical pulse with respirations, hypotension, jugular vein distension, muffled cardiac sounds, decreased QRS amplitude on electrocardiogram (ECG) |
46 | What are the four basic classifications of shock? | • Hypovolemic shock: Loss of blood volume • Obstructive shock: Decreased circulation resulting from external or intrinsic compression • Septic shock: Related to vascular dilation • Cardiogenic shock: Impaired perfusion from lack of sufficient cardiac output |
47 | What is the formula describing the rate of fluid maintenance for the pediatric patient? | The 4:2:1 rule = 4 mL/kg hourly for the first 10 kg, adding 2 mL/kg per hour for the second 10 kg, and adding 1 mL/kg per hour for each kilogram over 20 kg |
48 | What is the formula used to calculate the rate of fluid resuscitation of a burn victim? | The Parkland formula: Fluid for the first 24 hours (milliliter) = 4 x patient weight (kg) x % body surface area involved; the first half is given over 8 hours, the second half over the remaining 16 hours. Rule of 9’s for determining percentage of burned: 9% = head, each arm; 18% = chest, back, each leg |
What preoperative condition is associated with immunosuppression, poor wound healing, decreased basal metabolic rate, longer hospitalization, and an increased mortality rate? | Preoperative malnutrition | |
50 | Why should gastric residuals be checked every 4 hours in a patient receiving enteral nutrition via tube feeds? | Regurgitation and aspiration are risks of tube feeding |
51 | What is involved in the refeeding syndrome that is observed in severely malnourished patients following initiation of feeds? | Malnourishment leads to hypoinsulinemia and electrolyte abnormalities including intracellular hypophosphatemia. Within 4 to 5 days of reinitiation of carbohydrate metabolism and subsequently increased insulin production, patients can develop severe hypophosphatemia. |
52 | You are rounding on a patient who underwent major surgery for polytrauma and required 20 units of packed red blood cells. The patient is complaining of perioral numbness and tingling. What is the likely diagnosis and treatment? | Citrate toxicity with subsequent hypocalcemia. Treat with calcium gluconate. This should be given for symptomatic patients only. |
53 | What medications can be given as pretreatment to prevent mild hypersensitivity and nonhemolytic febrile reactions in a patient receiving blood transfusion with a history of mild reactions? | Acetaminophen and antihistamines such as diphenhydramine |
54 | What complications may be encountered in a patient who has received massive intraoperative transfusions? | Volume overload, hyperplasia or hypokalemia, hyperammonemia, acidosis, thrombocytopenia, coagulation factor depletion, coagulopathy, hypothermia, transfusion related acute lung injury, and citrate toxicity |
55 | What is transfusion-related acute lung injury? | Acute respiratory distress and noncardiogenic pulmonary edema that develops during or within 6 hours of blood transfusion. Treatment includes supportive measures, often including mechanical ventilation, high-inspired oxygen, and positive end expiratory pressures. |
56 | Mechanical ventilation is most commonly delivered via positive-pressure ventilation (PPV). What are the two most common subtypes of PPV that focus on the transition from inspiration to expiration? | • Volume control: A set volume is delivered per breath • Pressure control: A set pressure is delivered per breath |
57 | What common rule can be used to select the tidal volume and rate for a patient on assist control mechanical ventilation? | 12–12 rule: 12 mL/kg of lean body mass delivered 12 times a minute. It is useful for patients without preexisting lung disease. It must be adjusted for patients with known chronic obstructive pulmonary disease (COPD), etc. |
58 | What technique can be used in mechanical ventilation to maintain a patient’s airway pressure above atmospheric pressure at the end of expiration? | Positive end expiratory pressure (PEEP) |
59 | What is the difference in the 1-second forced expiratory volume FEV1 to vital capacity (FVC) ratio in COPD compared with that in restricted lung disease? | In COPD, the FEV1/FVC ratio decreases, whereas the ratio is preserved or increased in restrictive lung disease. |
60 | Describe the difference between the two types of postobstructive pulmonary edema. | • Type 1. Follows an acute severe cause of upper airway obstruction (epiglottitis, laryngospasm, strangulation) and usually manifests within 1 hour of the event • Type 2. Follows relief from a chronic obstruction (obstructive sleep apnea (OSA), choanal stenosis, subglottic stenosis) and usually manifests within 6 hours of reversing the obstruction |
What is the treatment of postobstructive pulmonary edema? | Oxygen and supportive care in mild cases and PEEP in more severe cases. Diuretic therapy can be instituted, although the benefit is not clear. | |
62 | What is the most common cause of fever in the immediate postoperative period? | Within the first 48 hours of surgery, fever is likely due to an inflammatory reaction to surgical insult or reaction to medication or blood product given intraoperatively. It is unlikely to be infectious. Evaluate for possible source of infection, but prophylactic antibiotics are not indicated. Patient may be treated with antipyretic and monitor for change in clinical status. |
63 | In the acute postoperative setting, how can the mnemonic “Wind, Water, Walk, Wound, Wonder Drugs, What did you do?” help in the evaluation of a febrile patient? | • Wind: Pneumonia? Aspiration? Atelectasis? • Water: Urinary tract infection? • Walk: Thrombophlebitis? Deep venous thrombosis? Pulmonary embolus? • Wound: Surgical-site infection? • Wonder drugs: Drug reaction (β-lactam antibiotic? Sulfa antibiotic?) • What did we do? Catheter-related infection? IV site infection? |
Otolaryngologic Manifestations of Systemic Disease
64 | What is eosinophilic granuloma? | Eosinophilic granuloma is the most common form of Langerhans cell histiocytosis and is characterized by the formation of solitary or multiple discrete nodules within bones. |
65 | What is Hand-Schüller-Christian disease? | It is multifocal Langerhans cell histiocytosis with bone “granulomas,” associated with the triad of exophthalmos, lytic skull lesions, and diabetes inspidus. |
66 | True or false. Most patients with Langerhans cell histiocytosis have multisystem disease. | False. Approximately two-thirds of patients have disease involving one site. |
67 | What is Letterer-Siwe disease? | Systemic Langerhans cell histiocytosis is the rarest (~ 10% of cases) and the most severe form of disease. Initial symptoms often include generalized skin eruption, anemia, and hepatosplenomegaly. |
68 | Extranodal natural killer cell (NK)/T-cell lymphoma, nasal type, is commonly associated with which virus? | Epstein-Barr virus |
69 | How is extranodal NK/T-cell lymphoma, nasaltype, commonly treated? | Chemotherapy (CHOP: cyclophosphamide, doxorubicin, vincristine, prednisone) in conjunction with radiotherapy |
70 | Compared with other types of lymphoma involving the head and neck, what is the prognosis for extranodal NK/T-cell lymphoma, nasal type? | Much poorer |
71 | What is the most common laryngeal manifestation of Wegener granulomatosis? | Subglottic stenosis |
72 | What is the most common otologic manifestation of Wegener granulomatosis? | Serous otitis media |
73 | What histopathologic findings are seen in Wegener disease? | Necrotizing granulomas and arteritis involving small vessels |
74 | What laboratory test is used to diagnose and follow Wegener disease? | Antineutrophil cytoplasmic antibody (C-ANCA). Test will be positive in more than 90% of cases. |
75 | What histopathological findings are seen in sarcoidosis? | Noncaseating granulomas |
76 | What condition is characterized by uveitis, parotid swelling, fever, and facial nerve palsy? | Heerfordt syndrome (uveoparotid fever), a manifestation of sarcoidosis |
What is the most common site of laryngeal involvement of sarcoidosis? | Supraglottis | |
78 | What is the most common head and neck manifestation of sarcoidosis? | Cervical lymphadenopathy |
79 | Describe a common presentation for pyogenic granuloma. | Less than 1-cm lobular red or purple lesion that develops on the gingiva or nasal mucosa that is friable and prone to bleeding. It occurs more commonly in women and is associated with trauma and pregnancy. |
80 | Describe the treatment of pyogenic granuloma. | Lesions frequently resolve spontaneously when associated with pregnancy. If frequent bleeding or cosmesis is a concern, conservative cauterization or excision can be pursued. |
81 | Describe the natural history of untreated necrotizing sialometaplasia. | Spontaneous resolution over weeks to months |
82 | How does blastomycosis typically manifest? | A common triad includes cutaneous disease, pulmonary involvement, and constitutional symptoms. Skin lesions may involve the face with verrucous growth and scarring. Oropharyngeal and laryngeal involvement are rare. |
83 | Describe the clinical manifestations of coccidiomycosis. | It is the cause of “valley fever.” Most patients have an influenza-like illness that includes malaise, fever, myalgia, arthralgia, and cough. Initial symptoms are pulmonary, mucocutaneous involvement with maculopapular rash, cervical lymphadenopathy, and/or meningeal involvement. |
84 | Where is Coccidioides immitis endemic? | Desert Southwest including New Mexico, Nevada, California, Texas, Utah, and northern Mexico |
85 | Histoplasmosis most commonly occurs in which geographic location? | The Ohio, Missouri, and Mississippi River valleys |
86 | Describe the head and neck manifestations of disseminated histoplasmosis. | Granulomatous lesions involving the lips, gingiva, tongue, larynx, and pharynx manifesting with painful ulcers containing heaped edges |
87 | What is the most common site of laryngeal involvement of histoplasmosis? | Supraglottis |
88 | How is histoplasmosis diagnosed? | Histoplasma antibody latex agglutination test, fungal stains, blood or urine antigens using enzyme-linked immunosorbent assay or polymerase chain reaction (PCR), or histoplasma skin test |
89 | What pathogen is responsible for the development of rhinosporidiosis? | The parasite Rhinosporidium seeberi |
90 | What are the common head and neck clinical manifestations of rhinosporidiosis? | Fleshy, friable strawberry-like lesions most commonly involving the inferior turbinate, oropharynx, conjunctiva, and perineum |
91 | What is the treatment for rhinosporidiosis? | Wide local excision or prolonged dapsone therapy |
92 | What is the causative organism in syphilis? | The spirochete Treponema pallidum |
93 | What is the treatment of syphilis? | Penicillin G benzathine |
94 | Describe the presentation of primary syphilis. | A painless ulcer (chancre) at the site of transmission demonstrating a rolled edge and punched-out base is present after 3 to 6 weeks at the site of exposure. |
95 | Describe the presentation of secondary syphilis. | Secondary syphilis is characterized by systemic spread of disease with manifestations including fever, myalgias, arthralgias, and lymphadenopathy. A mucocutaneous rash often develops including the oral mucosa and the palms and soles. Finally, condyloma lata and patchy alopecia may develop. |
What are the three categories of tertiary syphilis? | The three categories are gummatous syphilis, cardiovascular syphilis, and neurosyphilis. | |
97 | Describe the findings of congenital syphilis. | “Snuffles” with sinonasal drainage, saddle nose, saber shins, Hutchinson teeth, and mulberry molars |
98 | Describe the Argyll-Robertson pupil. | A pupil that does not react to light but does constrict during accommodation. Associated with syphilis |
99 | Describe the manifestation of otosyphillis. | Otosyphilis is associated with either congenital or tertiary acquired syphilis and manifests with sensorineural hearing loss beginning in the high frequencies, fluctuating tinnitus, and vertigo. |
100 | What is the Hennebert sign? | Rotary nystagmus when positive or negative pressure is applied to the tympanic membrane |
101 | Describe the Jarisch-Herxheimer reaction. | After treatment of syphilis, dying spirochetes may trigger a cytokine cascade that manifests with myalgias, fever, headache, and tachycardia. |
102 | What tests are commonly used for syphilis screening? | Venereal Disease Research Laboratory (VDRL), rapid plasma reagin (RPR) test |
103 | What confirmatory test should be ordered after a positive or equivocal screening test for syphilis? | FTA-ABS |
104 | What is the most common cause of subacute pediatric cervical lymphadenopathy? | Atypical Mycobacterium, most commonly M. avium–intracellulare, M. haemophilum, and M. scrofulaceum |
105 | How is brucellosis transmitted? | It is transmitted from contaminated meat or dairy products or via direct contact through broken skin. |
106 | What are the clinical manifestations of cat-scratch disease? | The primary lesion develops as an erythematous, nonpruritic pustule 1 week affter inoculation. Lymphadenitis of the axilla, neck, and inguinal region commonly develops 2 to 4 weeks after exposure. Suppuration with acute tenderness and fever frequently occurs. Lymphadenopathy usually resolves over 2 weeks but may persist for up to 2 years. |
107 | What are the pathogens associated with leprosy (Hansen disease)? | Mycobacterium leprae and Mycobacterium lepromatosis |
108 | What is the treatment for Hansen disease? | Dapsone |
109 | What pathogen is responsible for the development of rhinoscleroma? | Klebsiella rhinoscleromatis |
110 | What histologic findings are strongly suggestive of the diagnosis of rhinoscleroma? | Russell bodies (immunoglobulin containing inclusions in plasma cells), pseudoepitheliomatous hyperplasia, Mikulicz cells (foamy histiocytes containing Klebsiella) |
111 | What is the treatment for rhinoscleroma? | Tetracycline or ciprofloxacin |
112 | What tests are helpful in diagnosing systemic lupus erythematosus? | Antinuclear antibody (ANA), anti-Sm, anti-DNA, anti-ribo-nuclear protein (anti-RNP), and anticardiolipin antibody |
113 | What are the typical clinical manifestations of a patient with mixed connective tissue disease? | Raynaud phenomenon, arthralgias, inflammatory myopathy, lymphadenitis, skin or mucosal lesions, and serositis |
114 | What is the definition of mixed connective tissue disease? | Mixed connective tissue disease is characterized by a combination of overlapping features of systemic lupus erythematous, scleroderma, and polymyositis. Patients may manifest Raynaud phenomenon, arthralgias, inflammatory myopathy, lymphadenitis, skin or mucosal lesions, and serositis. |
115 | Which joints in the head and neck are most commonly affected by rheumatoid arthritis (RA)? | RA can affect any diarthrodial joint, including the temporomandibular, cricoarytenoid, and ossicular joints. |
What does the acronym CREST stand for? | Calcinosis, Raynaud phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasias. CREST syndrome is a limited cutaneous form of systemic scleroderma. | |
117 | What are the histologic findings in a minor salivary gland lip biopsy performed in a patient with Sjogren disease? | Focal lymphocytic infiltrate with atrophic acini |
118 | What head and neck sites are commonly affected by relapsing polychondritis? | Ear, nasal septum, and larynx |
119 | What is the most common head and neck manifestation of relapsing polychondritis? | Episodic auricular chondritis, presenting with erythema and pain of the pinna with sparing of the fatty lobule. Eventually presents in ~ 90% of patients |
120 | What are common symptoms of giant cell arteritis? | Headache (predominantly temporal region), jaw claudication (~ 50% patients), vision loss or visual disturbance, fatigue, general malaise, fever, anorexia, weight loss, night sweats, and tongue pain |
121 | What histologic finding on temporal artery biopsy is suspicious for giant cell arteritis? | Inflammatory infiltrates in at least the adventitia and media, with elastic lamina fragmentation |
122 | What imaging study may be useful in the diagnosis of giant cell arteritis? | Duplex ultrasound. High-resolution MRI has been reported to have very similar diagnostic power, but more data are needed before it can be recommended as a diagnostic tool. |
123 | What is the classic triad of Wegener granulomatosis? | Granulomas of the respiratory tract, progressive glomerulonephritis, and necrotizing vasculitis of small to mediumsized arteries and veins |
124 | What condition is characterized by uveitis, oral aphthous ulcers, and genital ulcers? | Behçet disease |
Neck Space Anatomy
125 | What are the two primary fascia networks of the neck? ( | Superficial cervical fascia and the deep cervical fascia |
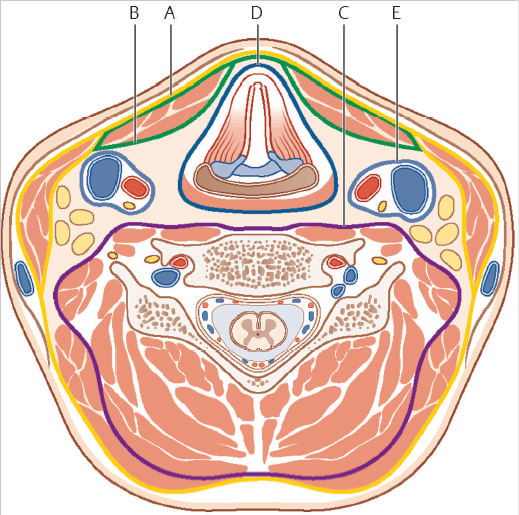
Fig. 4.2 Layers of the cervical fascia at level of C5 vertebra: (A) superficial cervical fascia; (B) muscular layer of the middle cervical fascia, (C) prevertebral fascia, (D) visceral layer of the middle cervical fascia, and (E) carotid sheath. (Used with permission from Behrbohm H, Kaschke O, Nawka T, Swift A. Ear, Nose, and Throat Diseases: With Head and Neck Surgery. New York, NY: Thieme; 2009.)
Describe the anatomy of the superficial cervical fascia. | It lies just deep to the dermis and superficial to the deep cervical fascia. It extends from the zygoma to the clavicle and envelops the platysma and muscles of facial expression. | |
127 | Describe the anatomy of the deep cervical fascia. | It is composed of the superficial (investing), middle (visceral and muscular), and deep (prevertebral and alar) layer. The carotid sheath fascia is created by all three layers of the deep cervical fascia. |
128 | Describe the anatomy of the superficial (investing) layer of the deep cervical fascia. | It surrounds the neck and inserts superiorly at the nuchal ridge, mastoid, zygoma, and mandible and inferiorly at the clavicles, sternum, scapula, and acromion. It envelops the sternocleidomastoid muscle, trapezius, muscles of mastication, submandibular glands, and parotid gland. Inferiorly, its manubrial insertion splits to form the suprasternal space of Burns. |
129 | Describe the anatomy of the middle (visceral and muscular) layer of the deep cervical fascia. | It extends superior to the cranial base and inferiorly to the upper mediastinum. It is subdivided into the muscular and visceral layers. The muscular division surrounds the infrahyoid strap muscles; the visceral portion surrounds the pharyngeal constrictors, esophagus, trachea, and thyroid and creates the buccopharyngeal fascia. Both divisions contribute to the carotid sheath. |
130 | Describe the anatomy of the deep (prevertebral and alar) layer of the deep cervical fascia. | It is subdivided into the alar and prevertebral fascia. Both extend superiorly from the cranial base, but the alar fascia fuses with the middle cervical fascia and extends into the upper mediastinum, and the prevertebral fascia extends to the level of the coccyx. The alar fascia and prevertebral fascia fuse at the vertebral transverse processes and after joining, envelop the paraspinous muscles. |
131 | Describe the anatomy of the suprasternal space (space of Burns). | The inferior insertion of the superficial (investing) fascia splits just above the manubrium attaching anterior to the manubrium and posteriorly to the interclavicular ligament. This small potential space contains a portion of the anterior jugular veins, and the sternal heads of the sternocleidomastoid muscle. |
132 | Define the boundaries of the buccal space. | The buccal space is created by the buccinator muscle medially; the superficial layer of the deep cervical fascia and the muscles of facial expression laterally and anteriorly; and the muscles of mastication, mandible, and parotid gland posteriorly. It primarily contains adipose tissue (buccal fat pad), minor salivary glands, accessory parotid tissue, and facial/buccal arteries, veins, and lymphatics. The buccal fat pad is pierced by the parotid duct as it courses to the buccinator and eventually enters the mouth opposite the second upper molar. |
133 | Define the mechanism of spread of infection (or tumor) to and from the buccal space. | It permits spread between the mouth, parotid space, and masticator space from deficient fascial compartmentalization along the superior, inferior, and posterior limits. |
134 | Define the boundaries of the carotid space. | The carotid sheath contains the carotid artery, internal jugular vein, vagus nerve, and jugular lymphatic chain. All three divisions of the deep cervical fascia form the carotid sheath. It extends from the skull base to the mediastinum; anteriorly lies the sternocleidomastoid muscle, posteriorly the prevertebral space, and medially the visceral compartment. |
135 | Review the risk factors for carotid blowout. | Radiation, salivary fistula, malnutrition, hypothyroidism, Tincision over the great vessels, radical neck dissection |
Define the boundaries of the danger space. | The danger space is a potential space that rests between the alar fascia and the prevertebral fascia. Infections in this area can communicate with the thorax (mediastinum) to the level of the diaphragm. |



