Purpose
To correlate visual acuity to macular spectral-domain optical coherence tomography (SD OCT) anomalies detected in children with a history of retinopathy of prematurity (ROP).
Design
Retrospective cohort study.
Methods
All charts of children with a history of ROP between 2 and 18 years of age and with SD OCT performed between 2010 and 2012 were reviewed. Central foveal thickness was measured and correlated with visual acuity. Secondary outcome measures included temporal parafoveal thickness, presence of the inner nuclear layer and outer segment, gestational age at birth, sex, spherical equivalent, history of laser treatment, and developmental delay.
Results
The study included 44 better-seeing eyes of 44 patients. Sixty-four percent (28/44) of patients in our study had 20/40 or better visual acuity despite an abnormal foveal morphology in 91% of total eyes.
Conclusion
Patients with a history of ROP demonstrate a high frequency of macular morphologic abnormalities, including retention of inner retinal layers and absent foveal depression, on SD OCT. These structural changes do not always correlate to visual acuity. Instead it appears that cone maturation may be a better indicator of visual acuity. In addition, there is a significant correlation between best-corrected visual acuity and myopia.
Retinopathy of prematurity (ROP) is a preventable and a potentially blinding disease that is becoming more prevalent as neonatal services improve. ROP is associated with a higher incidence of myopia, amblyopia, retinal detachment, strabismus, cataracts, vessel dragging, macular folds, and glaucoma. Macular edema, retention of inner retinal layers at the foveal center, and absence of a foveal depression have been reported in patients with ROP using optical coherence tomography (OCT). However, the clinical relevance of these findings remains unknown. Few studies have evaluated ROP maculopathy and some are limited by the use of traditional time-domain OCT.
The purpose of our study is to correlate visual acuity and macular spectral-domain (SD) OCT findings in children with a history of ROP.
Materials and Methods
An institutional review board–approved retrospective cohort study was performed at the Bascom Palmer Eye Institute, University of Miami Miller School of Medicine. A chart review of all children with a history of ROP between 2 and 18 years of age and with SD OCT (Heidelberg Engineering, Heidelberg, Germany) performed between 2010 and 2012 was conducted. Patients were identified by their International Classification of Diseases (ICD-9) code. All eyes with a history of intraocular surgery, poor OCT image quality, and abnormal funduscopy such as macular dragging, macular folds, or retinal detachment were excluded from study. Only the eye with best-corrected visual acuity from each patient was included to minimize the effect of amblyopia. Data regarding gestational age at birth, sex, spherical equivalent, best-corrected visual acuity, history of laser, and developmental delay were recorded.
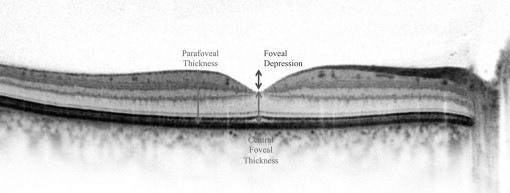
OCT scans were reviewed and manually centered. The scan line through the foveal center of the macular cube was used for data measurements. The central foveal thickness and the nasal and temporal parafoveal thickness were measured. The mean of the parafoveal thickness measurements was calculated. The foveal depression was calculated by subtracting the central foveal thickness from the mean parafoveal thickness ( Figure 1 ). Values less than 56.4 μm were considered to be indicative of absence of a foveal depression. The presence of the inner nuclear layer and outer segment elongation at the center of the fovea was also evaluated.
Subjects were divided by visual acuity into Group 1 (visual acuity 20/40 or better) and Group 2 (visual acuity worse than 20/40). Statistical analysis was performed using χ 2 and Student t test.
Results
The study included 44 eyes of 44 patients. Overall, the study population had a mean visual acuity 0.30 ± 0.20 logMAR, mean age of 8.8 ± 3.7 years, gestational age of 25.1 ± 2.2 weeks, laser treatment in 36 eyes (82%), and spherical equivalent −7.1 ± 6.8 diopters (D). On OCT analysis, the mean central foveal thickness was 305 ± 33 μm, mean parafoveal thickness was 329 ± 27 μm, and mean foveal depression was 19.2 ± 25.1 μm. A foveal depression was absent in 40 eyes (91%) and the inner nuclear layer was present in the center of the fovea in 26 eyes (59%). Outer segment elongation was present in 42 eyes (95%). When divided by the visual acuity, Group 1 included 28 eyes (64%) and Group 2 included 16 eyes (36%).
Group 1 consisted of 28 eyes with a mean age of 9.4 ± 4.0 years, gestational age of 24.9 ± 1.7 weeks, laser treatment in 20 eyes (71%), and spherical equivalent −5.5 ± 6.5 D. The mean central foveal thickness was 309 ± 34 μm, mean parafoveal thickness was 336 ± 34 μm, and mean foveal depression was 21.8 ± 29 μm. A foveal depression was absent in 24 eyes (86%), the inner nuclear layer was present in the center of the fovea in 15 eyes (54%), and outer segment elongation was identified in 100% of eyes.
Group 2 consisted of 16 eyes with a mean age of 7.9 ± 2.8 years, gestational age of 25.6 ± 2.9 weeks, laser treatment in 16 eyes (100%), and spherical equivalent −10.0 ± 6.7 D. The mean central foveal thickness was 297 ± 30 μm, mean parafoveal thickness was 321 ± 16 μm, and mean foveal depression was 16.3 ± 22 μm. A foveal depression was absent in all eyes and the inner nuclear layer was present in the center of the fovea in 11 eyes (69%). Elongation of the outer segment was identified in 88% of eyes.
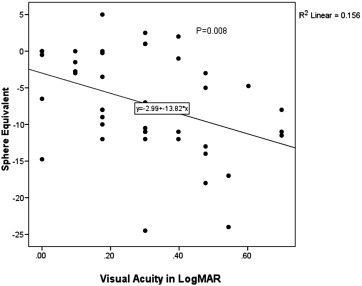
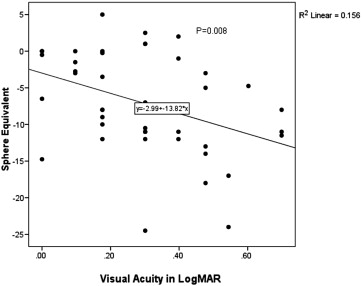
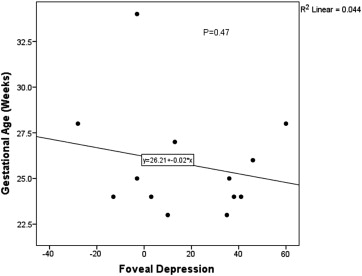
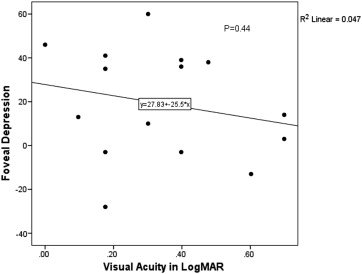
Statistical analysis was performed between the 2 groups. Older children had significantly better visual acuity than younger children ( P value = .04). Myopia was significantly higher in Group 2 ( P = .04). The spherical equivalent was highly correlated to visual acuity ( Figure 2 ). Cognitive delay was not statistically different among groups. All eyes had laser treatment in Group 2; however, only 71% had laser in Group 1 ( P value = .02). Children born at 26 weeks gestational age or younger were more likely to have had laser treatment ( P value = .03). Absence of a foveal depression did not correlate to gestational age or visual acuity ( Figures 3 and 4 ); however, the majority of patients in the study (42/44) were younger than 28 weeks gestational age at birth.
Results
The study included 44 eyes of 44 patients. Overall, the study population had a mean visual acuity 0.30 ± 0.20 logMAR, mean age of 8.8 ± 3.7 years, gestational age of 25.1 ± 2.2 weeks, laser treatment in 36 eyes (82%), and spherical equivalent −7.1 ± 6.8 diopters (D). On OCT analysis, the mean central foveal thickness was 305 ± 33 μm, mean parafoveal thickness was 329 ± 27 μm, and mean foveal depression was 19.2 ± 25.1 μm. A foveal depression was absent in 40 eyes (91%) and the inner nuclear layer was present in the center of the fovea in 26 eyes (59%). Outer segment elongation was present in 42 eyes (95%). When divided by the visual acuity, Group 1 included 28 eyes (64%) and Group 2 included 16 eyes (36%).
Group 1 consisted of 28 eyes with a mean age of 9.4 ± 4.0 years, gestational age of 24.9 ± 1.7 weeks, laser treatment in 20 eyes (71%), and spherical equivalent −5.5 ± 6.5 D. The mean central foveal thickness was 309 ± 34 μm, mean parafoveal thickness was 336 ± 34 μm, and mean foveal depression was 21.8 ± 29 μm. A foveal depression was absent in 24 eyes (86%), the inner nuclear layer was present in the center of the fovea in 15 eyes (54%), and outer segment elongation was identified in 100% of eyes.
Group 2 consisted of 16 eyes with a mean age of 7.9 ± 2.8 years, gestational age of 25.6 ± 2.9 weeks, laser treatment in 16 eyes (100%), and spherical equivalent −10.0 ± 6.7 D. The mean central foveal thickness was 297 ± 30 μm, mean parafoveal thickness was 321 ± 16 μm, and mean foveal depression was 16.3 ± 22 μm. A foveal depression was absent in all eyes and the inner nuclear layer was present in the center of the fovea in 11 eyes (69%). Elongation of the outer segment was identified in 88% of eyes.
Statistical analysis was performed between the 2 groups. Older children had significantly better visual acuity than younger children ( P value = .04). Myopia was significantly higher in Group 2 ( P = .04). The spherical equivalent was highly correlated to visual acuity ( Figure 2 ). Cognitive delay was not statistically different among groups. All eyes had laser treatment in Group 2; however, only 71% had laser in Group 1 ( P value = .02). Children born at 26 weeks gestational age or younger were more likely to have had laser treatment ( P value = .03). Absence of a foveal depression did not correlate to gestational age or visual acuity ( Figures 3 and 4 ); however, the majority of patients in the study (42/44) were younger than 28 weeks gestational age at birth.