(1)
Alo Eye Care, Kolkata, India
Keywords
Advancement flapBurow’s trianglesMonopedicle flapBipedicle flapV-Y plastyRotation flap‘Z’–plastyRhomboidDufourmental FlapsBilobed Flaps9.1 Introduction
A flap is a unit of tissue transferred from one site (donor site) to another (recipient site) while maintaining its own blood supply. Flaps come in many different shapes and forms. They range from simple advancements of skin to composites of many different types of tissue. These composites need not consist only of soft tissue; they may include skin, muscle, bone, fat, or fascia. Because this chapter deals only with lid reconstruction, our discussion is limited mainly to skin and underlying soft tissue flaps.
Flaps and their mobilization form the basis of almost all lid reconstruction procedures. If the surgeon cannot visualize from where and how he or she will fill the lid tissue defect, the technique and outcome will not be satisfactory. If necessary, the surgeon should sketch the tissue defect on paper, consider all the options, and then choose one. Regardless of the approach selected, the surgeon should mobilize the flap very liberally so that there is no undue tension on the apposition suture line.
9.2 Advancement Flaps
9.2.1 Introduction
An advancement flap allows for “sliding movement” of the incised tissue. The flap advances from the adnexal tissue to cover the primary defect.
9.2.2 Technique
The basic principle is to extend the incision along parallel lines on the sides of the defect. The flap is undermined completely from the deeper tissue. The mobilized tissue is pulled over the primary defect to cover it. Care is taken to avoid undue tension on the suture line, as it may give way. If necessary, a bit more mobilization and undermining may be done. The flap is sutured to the margin of the defect with either 5/0 silk or Nylon interrupted sutures. With mobilization of a long flap, there is risk of a dog ear deformity at the extreme end of the flap. Management of this deformity is discussed later.
9.2.3 Other Variations/Options
The classically designed advancement flap has a length-to-width ratio of around 1:2 and advances tissue a distance approximating the width of the flap. Advancement beyond this point is possible, almost up to 1:4, but the tension on the flap may increase dramatically and the distal blood flow may become compromised, leading to distal flap necrosis.
These flaps are particularly useful for forehead and brow defects because the relaxed skin tension lines (RSTLs) in this region are horizontal and parallel. Although the classic advancement flap has two parallel sides, modifications of this flap are easy to design based on the position of the RSTLs and along skin crease lines, especially for the periocular skin.
Not all advancement flaps are purely advancement. The cheek advancement flap is primarily a sliding or advancement flap but also relies on rotation.
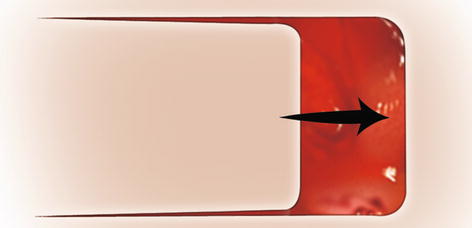
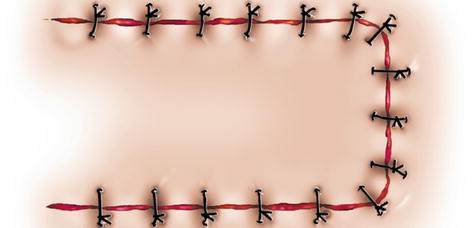
Fig. 9.1
Advancement flap. Mobilization of the advancement flap
Fig. 9.2
Advancement flap. The tissue defect has been covered by the mobilized flap
9.3 Burow’s Triangle
9.3.1 Introduction
Burow’s triangle is a clump of residual excess tissue in the form of a dog’s ear, formed when long advancement flaps are used. Excision of this tissue may facilitate movement of the flap and reduces cosmetically unpleasing redundant tissue. A Burow triangle, or dog ear deformity, should never be excised before the flap is advanced into position, because redundancy may be minimal and resection may be unnecessary.
9.3.2 Management Technique
Once the surgeon reaches the end of the advancement edge, and if the advancement is quite long, he or she determines whether a fold of redundant skin exists. This tissue is lifted by pinching it with a tooth forceps. With either a sharp blade or scissors, it is cut from the skin. The resultant skin margin is apposed with interrupted stitches.
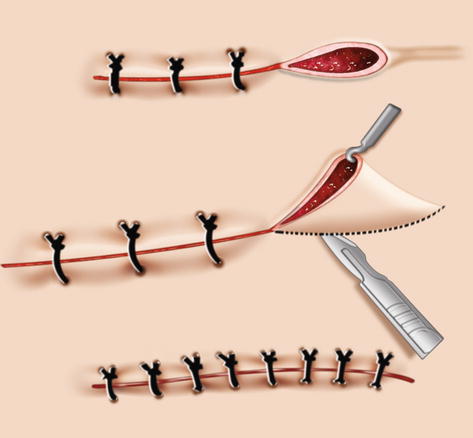
Fig. 9.3




Burow’s triangles. At the end of an advancement flap, an excess redundant tissue fold is formed (top). The redundant tissue is lifted with forceps, and the tissue is excised from the base (middle). The resulting cut margin is repaired with interrupted sutures (bottom)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
