The femtosecond laser represents a significant advance in the field of refractive surgery. Mechanical microkeratomes were the only instruments available for flap creation in the early days of LASIK. In 2001, the FDA approved the first femtosecond laser for the LASIK flap. The use of the femtosecond laser has steadily increased since then. By 2010, over 50% of the LASIK procedures in the United States were performed with the femtosecond laser. Significant improvements in femtosecond technology have occurred over the last decade. In addition to flap creation, the lasers can be used to create channels for intrastromal rings, and can be used for keratoplasty and cataract surgery. IntraLase Corporation of Irvine, California, developed the first commercially available femtosecond laser. Lasers that are FDA approved and currently in use at this time include: Abbott Medical Optics IntraLase FS and iFS, Alcon WaveLight FS200, Carl Zeiss Meditec VisuMax, Technolas Perfect Vision 520F, and Ziemer Ophthalmic Systems Femto LDV.
▪ Laser Physics
The femtosecond laser is a focusable infrared laser similar to the Nd-YAG (neodymium-yttrium-aluminum-garnet) laser used for the posterior capsulotomy procedure; however, this laser delivers ultrashort laser pulses, firing in the femtosecond duration range (100 × 10-15 second). The advantage of a femtosecond laser is that the extremely short laser pulse of focused energy causes minimal thermal damage or disruption in adjacent tissues. This adjacent disruption in the corneal stroma has been measured and extends out on the order of 1 µm. The femtosecond laser pulse vaporizes small amounts of tissue by the process of photodisruption. The vaporized tissue forms an intrastromal cavitation bubble of microplasma, which is composed of water and carbon dioxide. Focusing the laser energy at a specified tissue depth and placing successive laser spots in close proximity to one another, multiple bubbles are created in a lamellar corneal dissection plane. Some lasers create the dissection plane using a raster (zigzag) line pattern, while others use a spiral pattern. The laser-controlled software can be programmed by the surgeon to create lamellar, axial (side cut), or pocket cuts in a wide range of depths and diameters. Typically after the lamellar cut has been completed, the side cut is created with a series of vertically placed spots along the flap edge.
Significant advances have been made with femtosecond technology over the last decade. First generation femtosecond lasers had repetition rates of approximately 15 kHz, and flap creation could take 60 to 90 seconds. Some current generation lasers operate in the 150 to 200 kHz range and have flap creation time of <10 seconds. Other lasers such as the Ziemer Femto LDV use very high pulse rate in the MHz range with lower energy per pulse. Despite the differences in laser dynamics and parameters from one laser to another, there are basic principles and practices that are applicable to all femtosecond lasers. The rest of the chapter will focus on the important clinical concepts that can be applied to any femtosecond laser platform used for LASIK flap creation.
▪ Advantages & Disadvantages of Femtosecond Lasers
The selection of candidates for LASIK with a femtosecond laser is similar in many respects to that for the blade microkeratome. First and foremost is patient safety, followed by the ability to meet patient expectations. However, femtosecond technology may expand the limits of candidacy for LASIK surgery. The advantages and disadvantages of the femtosecond laser for flap creation are summarized in Table 5.1.
Various studies have demonstrated that when compared to mechanical microkeratomes, femtosecond lasers create flaps with more predictable thickness. Femtosecond lasers can also create thinner flaps. The ability to create thinner flaps combined with tighter variance between expected and actual flap thickness may allow more patients with relatively thin corneas or highly myopic patients to undergo the procedure. Intraoperative pachymetry in such cases is still recommended prior to excimer ablation to ensure adequate residual stromal bed thickness.
TABLE 5.1 Summary of the Advantages and Disadvantages of Femtosecond Laser Flap Creation
Advantages
Disadvantages
Greater predictability of flap thickness; ability to create thinner flaps
High cost
Greater predictability of flap diameter
Need to acquire new skills
Flap creation independent of corneal contour or corneal diameter
Increased risk of inflammation (DLK)
Reduced incidence of button hole, partial flap, and intraoperative abrasion
TLSS or Good Acuity Plus Photosensitivity (GAPP); also Peripheral light spectrum phenomenon/Rainbow glare
Ability to retreat in the event of a suction break
OBL may interfere with excimer ablation
Epithelial sloughing of the flap is unlikely
Rarely intracameral bubbles can interfere with laser tracking, delaying surgery
Increased flap adherence long term reduces risk of traumatic flap displacement
Increased flap adherence makes flap lift for retreatment long term more difficult
Less bleeding from corneal neovascularization
Not suited to LASIK after RK or PK due to increased flap manipulation and potential wound disruption
Creation of a more planar flap
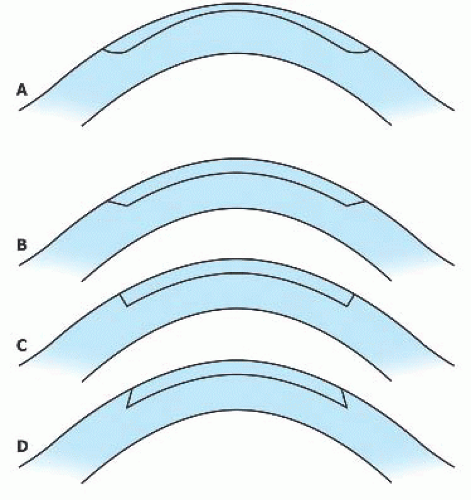
Femtosecond lasers also create more predictable flap diameters and shapes compared to flaps created with a microkeratome. With a mechanical microkeratome, patients with steeper corneas are at a higher risk for a buttonhole flap or a wider than anticipated flap diameter. Patients with flat corneas are at a higher risk for free flap or a smaller than anticipated flap diameter. With femtosecond lasers, the above mentioned complications are unlikely to occur even in patients with contours at the upper and lower ends of the normal range. Patients with smaller corneas can be treated with less risk of invading the sclera, because of the ability to better adjust flap diameter. Additionally, femtosecond lasers create flaps with a more desirable planar configuration and uniform thickness. Flaps created with a microkeratome have a meniscus shape with the flap periphery being thicker than the center (see Fig. 5.1). Most blade microkeratomes create thinner flaps on the second eye when the same blade is used for both eyes. They also create thinner flaps in thinner corneas and thicker flaps in thicker corneas. This is not the case with the femtosecond laser.
Femtosecond lasers are capable of creating more predictable and desirable side-cut profiles. With mechanical microkeratomes, the side-cut angle is more tapered or sloped. Femtosecond lasers allow the surgeon to specify the side-cut angle. The side-cut angle range varies with different laser manufacturers, but vertical, near-vertical, or reverse beveled angles can be created (refer to Fig. 5.1).
FIGURE 5.1 Mechanical microkeratomes cut a flap with a sloping side-cut angle and some cut a flap with a meniscus contour, i.e. thicker in the periphery and thinner in the center (A). In contrast, femtosecond lasers create a planar flap with an angled side cut (B), a perpendicular side cut (C), or a reversed beveled side cut (D).
Proposed mechanisms of epithelial ingrowth include a defect or gap at the flap margin facilitating epithelial migration under the flap, as well as seeding of the stromal bed during the microkeratome pass. Because sidecut angles created with the femtosecond laser are more vertical, the epithelium is less likely to migrate beneath the flap. This may explain the reduced likelihood of significant epithelial ingrowth following LASIK surgery using the femtosecond laser.
The angle on the side cut theoretically may make the flap more resistant to displacement soon after surgery, and now can be varied over a wide range, with some potential strength advantages to an inverted side cut that has an angle of more than 90 degrees. The flap is definitely more resistant to displacement 1 year after surgery; in fact, it may be difficult to lift the flap for retreatment.
▪ Femtosecond Laser Parameters
The surgeon has control over many of the flap parameters. Each type of laser has a particular range of adjustable parameters that can be manipulated by the surgeon. Despite the differences between lasers, an understanding of the common parameters and their impact on flap creation is necessary for a surgeon to optimize the femtosecond laser settings. The important parameters are flap thickness, bed energy, spot size and separation, flap diameter, hinge location, pocket profile, and side-cut angle/energy. It is wise to heed the recommendations of the representatives of the laser manufacturer and other more experienced surgeons when adjusting settings. As the surgeon gains more intraoperative experience, for example, trouble lifting the flap, and postoperative experience, such as inflammation or associated photophobia, fine-tuning adjustments can be made with various parameters to minimize side effects and facilitate flap creation. A summary of some of the parameters for current generation lasers is in Table 5.2.
FLAP THICKNESS
The surgeon can specify the flap thickness within the parameters of the given laser. The actual thickness of laser-made flaps measured by OCT or subtraction pachymetry comes closer to the intended thickness than does the thickness of flaps made with a microkeratome. It remains helpful intraoperatively to measure the stromal bed after the flap lift in order to calculate the anticipated post-ablation residual stromal bed.
BED ENERGY, SPOT SIZE
In general, the goal is to create a flap that is easy to lift using the lowest amount of energy. Insufficient energy will result in a flap that is harder to lift and possibly increase the chance of flap striae or flap tear. Excessive energy will increase the likelihood of postoperative inflammation, for example, diffuse lamellar keratitis (DLK) or Transient Light Sensitivity Syndrome (TLSS). The power of each spot can be adjusted and must be specifically set for each individual laser. Spot separation is the space between each laser spot that will create a cavitation bubble. Some lasers also permit the surgeon to specify the space between each line of laser spots created during the raster pattern treatment. Smaller spot separation or line separation will result in more laser spots being delivered during the procedure. Therefore, either an increase in bed energy or a decrease in spot or line separation will lead to more energy being delivered during the procedure. Conversely, a decrease in bed energy or increase in spot or line separation will lead to reduced energy being delivered during the procedure. Once power settings and spot or line separation are at desirable levels, they are usually not adjusted for each patient.
TABLE 5.2 Summary of Parameters of Various Currently Available Femtosecond Lasers Expand Transient Light Sensitivity Syndrome (TLSS)
Alcon WaveLight FS200
AMO IntraLase iFS
Carl Zeiss Meditec VisuMax
Technolas Perfect Vision 520F
Ziemer Femto LDV
Pulse rate
200 kHz
150 kHz
500 kHz
80 kHz
>5MHz
Side-cut angle (degrees)
30-150
30-150
45-135
60-120
28 (fixed)
Cone-cornea interface
Flat
Flat
Curved
Curved
Flat
Duration
300 fs
600-800 fs
220-580 fs
500-700 fs
200-350 fs
Wavelength
1,050 nm
1,053 nm
1,043 nm
1,053 nm
1,045 nm
Pulse energy
0.1-2.4 mJ
800-1,000 nJ
180-220 nJ
650-2,500 nJ
<100 nJ
Laser type
Amplifier
Amplifier
Amplifier
Amplifier
Oscillator
Ablation pattern
Raster
Raster
Spiral
Spiral
Raster
Only gold members can continue reading. Log In or Register to continue