Purpose
To assess the use of a new polygonal trephination pattern for penetrating keratoplasty (PK) assisted by femtosecond laser.
Design
Prospective, nonrandomized clinical study.
Methods
Sixteen eyes underwent decagonal PK. Nine had Fuchs dystrophy, 4 had pseudophakic bullous keratopathy, 1 had experienced trauma, 1 had corneal amyloidosis, and 1 had keratoconus. A Femtec (Tecnolas PerfectVision) laser was used to create decagonal penetrating cuts on both donor and recipient corneas. All patients were evaluated for uncorrected visual acuity, best spectacle-corrected visual acuity, pachymetry, topography, and endothelial cell density. Scanning electron microscopy was performed on corneal tissue after surgery.
Results
All eyes were treated successfully without intraoperative complications. The mean follow-up ± standard deviation was 9.75 ± 3.5 months. Mean postoperative best spectacle-corrected visual acuity was 20/53, and there was a significant improvement in both uncorrected visual acuity ( P = .0019) and best spectacle-corrected visual acuity ( P = .001). At 6 months, mean ± standard deviation manifest astigmatism was 1.90 ± 1.20 diopters. Mean endothelial cell density was 1502 ± 458 cells/mm 2 . Scanning electron microscopy displayed straight decagonal cut margins and minor remaining tissue bridges.
Conclusions
Use of the decagonal trephination profile was effective and safe to perform PK. Short-term visual results and refractive results are encouraging compared with those of conventional PK studies. Longer-term follow-up and comparative studies are necessary to determine precisely advantages the and optimal surgical settings of this technique.
Since the first human full-thickness corneal transplantation, performed by Zirm in 1906, penetrating keratoplasty (PK) has grown to be the most frequently performed tissue transplant in the world. Surgical improvements lead to a gradual change in procedures over the next several decades. High astigmatism is one of the major issues that can compromise a patient’s visual rehabilitation after PK. Numerous procedures have been tested to correct astigmatic errors, including relaxing procedures, wedge resections, and photorefractive procedures. Femtosecond laser is a step forward in the refinement of corneal surgery. By performing the same trephination profile on both donor and recipient tissue, laser-assisted surgery may improve wound adaptation and visual outcomes.
The femtosecond laser is a focusable infrared laser that delivers ultrashort pulses in the femtosecond duration range. Contiguous pulses are placed at a definite depth within the cornea, thus resecting only targeted tissue. This surgical device allows cutting of corneal tissue in a number of transplant designs and allows the use of sagittal plane trephination profiles, such as zigzag, top-hat, Christmas tree, and mushroom shapes to improve wound stability and to reduce postoperative astigmatism. The Technolas laser (Technolas PerfectVision, Heidelberg, Germany) can be used to create additional geometric configurations to increase the postoperative results of keratoplasty. Herein, we report outcomes of a decagonal-shaped PK cut profile using a femtosecond laser.
Methods
All surgeries were performed in our department from November 2007 through April 2008. All procedures were performed by one surgeon (H.P.). Corneal trephination was performed using a Technolas laser. This apparatus consists of a pulsed solid body (neodymium:glass) laser with a repetition rate of 40 kHz that emits light with a wavelength of 1055 nm and a pulse duration of 800 femtoseconds. The laser was set to obtain a decagonal corneal button of 8.0-mm decagonal trephination on donor tissue and an 8.0-mm decagonal trephination on recipient tissue. The cut rim angle was set at 90 degrees to the corneal surface tangent. Laser beam energy of 3.2 to 3.4 μJ and a spot separation of 3 μm were chosen. A double-pass procedure was used to reduce the amount of residual tissular bridges and to ease the opening of the wound (the first laser cut started from 1300 to 200 μm under the corneal surface and a second laser cut followed the same pattern up to the surface). Donor corneoscleral discs were mounted on an artificial anterior chamber (Moria, Anthony, France) filled with BSS plus (Alcon, Fort Worth, Texas, USA) up to a pressure of 20 mm Hg. Corneal thickness subsequently was determined by ultrasound pachymetry (UP-1000; Nidek, Tokyo, Japan). Corneoscleral discs were placed under the laser through a concave patient interface and were centered using the reflex image of the diode lights of the laser. After trephination, the corneal button was separated by blunt dissection with a Sinskey manipulator (Moria, Anthony, France). On the recipient, the procedure required placement of a suction ring. After a proper vacuum seal was obtained, the patient interface was applied and the laser procedure was performed as previously described. After completion of the cut, the eye was disconnected from the laser and the corneal button was removed by dissection with a blunt hook. The corneal graft then was positioned on the recipient eye after filling of the anterior chamber with a cohesive viscoelastic (Healon GV; AMO, Ettlingen, Germany) and was secured by a combination of 10 interrupted sutures on each angle of the decagon, then a 10-bite running suture was added on the middle of each decagon side. After surgery, patients received tobramycin plus dexamethasone eyedrops (TobraDex; Alcon) 3 times daily for 1 month and then slowly tapered. Selective suture removal was performed starting at the first-month visit if astigmatism was more than 3 diopters (D).
Postoperative examinations were planned at 7 days and at 1, 3, 6, 9, and 12 months. The following data were evaluated: uncorrected visual acuity, best spectacle-corrected visual acuity, slit-lamp biomicroscopy, and dilated fundus examination. All visual acuity data were converted to logarithm of minimal angle of resolution units. Statistical analysis was performed using SPSS software version 13.0 (SPSS, Inc, Chicago, Illinois, USA). The Wilcoxon rank-sum test was used to assess the difference between examinations. A P value < .05 was considered significant. Endothelial cell density and central corneal pachymetry were obtained by noncontact specular microscopy (Topcon SP-2000 and ImageNet Computerized Analysis System; Topcon, Tokyo, Japan).
Objective astigmatism, specular corneal topography, surface regularity index, surface asymmetry index, and the root mean square at 3 mm were evaluated using the OPD scan station (ARK 10000; NIDEK). All patients underwent anterior segment optical coherence tomography to evaluate wound alignment and suture configurations (Stratus OCT 3; Carl-Zeiss Meditec, Inc, Jena, Switzerland). All donor corneoscleral rims and recipients corneal buttons were fixed with 2.5% glutaraldehyde for scanning electron microscopy (Philips XL 30S, Amsterdam, The Netherlands).
Results
Sixteen eyes of 16 patients (7 men and 9 women) with a mean age ± standard deviation (SD) of 71.4 ± 20.1 years (range, 21 to 92 years) underwent decagonal penetrating keratoplasty. Mean follow-up ± SD was of 9.75 ± 3.5 months. Surgical indication was Fuchs dystrophy in 9 patients (56.25%), pseudophakic bullous keratopathy in 4 patients (25%), keratoconus in 1 patient (6.25%), trauma in 1 patient (6.25%), and corneal amyloidosis in 1 patient (6.25%). Preoperative examination showed 2 cases of age-related macular degeneration, 1 case of diabetic macular edema, and 1 case of epiretinal macular membrane.
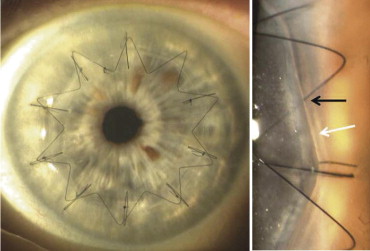
All procedures were uneventful. After surgery, 1 case of macular edema was diagnosed and 1 patient showed a retinal detachment at the third postoperative month and required subsequent surgery. Demographic and diagnostic data are summarized in Table 1 . A perfect wound apposition was observed in all cases, as illustrated in Figure 1 . An early and transient postoperative corneal edema was noted around the surgical wound after laser exposure; complete resolution was observed after 7 days. Epithelialization was completed after 3 days in all cases.
| Patient No. | Gender | Age (yrs) | Eye | Primary Diagnosis | Secondary Diagnosis |
|---|---|---|---|---|---|
| 1 | F | 82 | Left | Failed DSAEK | ARMD |
| 2 | M | 28 | Left | Corneal amyloidosis | None |
| 3 | F | 77 | Right | Pseudophakic bullous keratopathy | ARMD |
| 4 | M | 72 | Left | Fuchs dystrophy | Allograft rejection |
| 5 | F | 80 | Left | Failed DSAEK | None |
| 6 | F | 82 | Left | Fuchs dystrophy | None |
| 7 | M | 78 | Right | Pseudophakic bullous keratopathy | None |
| 8 | M | 55 | Left | Pseudophakic bullous keratopathy | None |
| 9 | F | 80 | Left | Fuchs dystrophy | None |
| 10 | F | 92 | Right | Fuchs dystrophy | None |
| 11 | M | 90 | Right | Fuchs dystrophy | Macular edema |
| 12 | M | 72 | Left | Trauma | Epiretinal membrane |
| 13 | M | 72 | Right | Fuchs dystrophy | Diabetic macular edema |
| 14 | F | 80 | Left | Fuchs dystrophy | None |
| 15 | F | 21 | Left | Keratoconus | None |
| 16 | F | 82 | Left | Pseudophakic bullous keratopathy | None |
Visual outcomes are summarized in Tables 2 and 3 . Significant differences between preoperative and postoperative uncorrected visual acuity and best spectacle-corrected visual acuity were observed ( P = .0019 and P = .0010, respectively). If the 5 cases of preoperative retinal impairment were excluded from the analysis, postoperative uncorrected visual acuity and best spectacle-corrected visual acuity would have been 20/54 ± 0.12 (range, 20/100 to 20/33) and 20/33 ± 0.10 (range, 20/50 to 20/25), respectively.
| Patient No. | Preoperative UCVA | Preoperative BSCVA | Postoperative UCVA | Postoperative BSCVA |
|---|---|---|---|---|
| 1 | 20000 | 20000 | 2000 | 2000 |
| 2 | 2000 | 200 | 63 | 32 |
| 3 | 2000 | 200 | 400 | 400 |
| 4 | 200 | 200 | 32 | 32 |
| 5 | 2000 | 2000 | 100 | 40 |
| 6 | 2000 | 160 | 50 | 40 |
| 7 | 2000 | 2000 | 63 | 25 |
| 8 | 60 | 50 | 50 | 30 |
| 9 | 200 | 200 | 50 | 50 |
| 10 | 2000 | 2000 | 63 | 25 |
| 11 | 2000 | 2000 | 100 | 100 |
| 12 | 400 | 133 | 40 | 40 |
| 13 | 200 | 133 | 400 | 63 |
| 14 | 2000 | 80 | 50 | 40 |
| 15 | 400 | 100 | 50 | 25 |
| 16 | 2000 | 2000 | 50 | 30 |
| Mean ± standard deviation (lines) | 20/783 ± 6 | 20/356 ± 7.1 | 20/82 ± 4.6 | 20/53 ± 5 |
| Variable | Mean UCVA | Mean BSCVA | ||
|---|---|---|---|---|
| LogMAR | Snellen | LogMAR | Snellen | |
| Initial examination | 1.59 ± 0.60 | 20/783 | 1.25 ± 0.71 | 20/356 |
| Final examination | 0.61 ± 0.46 | 20/82 | 0.42 ± 0.50 | 20/53 |
| P value | .0019 | .001 | ||
Refractive data for each patient are summarized in Table 4 . Mean ± SD postoperative spherical equivalent was 0.10 ± 1.83 D (range, −0.88 to 5.00 D). Mean ± SD manifest and topographic postoperative astigmatism were 1.90 ± 1.20 D (range, 0.00 to 5.00 D) and 3.10 ± 1.20 D (range, 0.89 to 5.73 D), respectively. Mean ± SD postoperative root mean square was 2.00 ± 1.29 D (range, 0.69 to 4.90 D), surface regularity index was 1.39 ± 0.36 (from 0.56 to 2.13), and the surface asymmetry index was 1.33 ± 0.80 (from 0.52 to 3.91). At 6 months, mean ± SD central corneal pachymetry and endothelial cell density were 508 ± 32 μm and 1502 ± 458 cells/mm 2 , respectively.



