8 Failures and Repeat Surgery
Indications
• Planned or involuntary two-stage operations
• Persistent or new disturbance of nasal respiration
• Persistent or recurrent sinusitis
• Olfactory disturbance
• Postoperative complications
• Surgical errors
• Inadequate aftercare
• Abnormal anatomical structure
• Systemic mucosal dysfunction
• Inappropriate habits and environment
Principles
Despite its popularity, endoscopic sinus surgery (ESS) is to the present day afflicted with suspicion of its being dangerous and, in the long term, somewhat unsuccessful, allegedly often requiring reoperation. The complications of ESS and their management will be touched upon in chapter 9 on trauma, while the reasons for failures and the principles of revision surgery will be analyzed in the following.
Confronted with the complaints of a previously operated patient, the rhinologist must analyze the symptoms and the postoperative history, including sociopsychological aspects, and then add a thorough endoscopic examination and possibly order a CT scan, a laboratory investigation for causative agents, and a medical diagnosis.
The indications for revision surgery, if not planned as complementary in a two-stage protocol, are based on these findings and suggested and supported by the patient’s presenting symptoms. The therapist devoted to the principle of causative treatment will, of course, try to identify and consider all possible causes of an unfortunate outcome–e. g., surgical mistakes, insuffi cient aftercare, abnormal anatomy, systemic mucosal defi ciency or inappropriate habits–and will endeavor to prevent further failures.
Reasons for Failures and Their Repair
Persistent or Recurrent Chronic Sinusitis
Persistent sinusitis after previous endoscopic sinus surgery is a major complaint of patients who continue or begin again to suffer from stuffy nose, hypersecretion, headache, asthmatic bronchitis, etc. Among this unsatisfied group are many who report an onset of the symptoms after a postoperative interval of weeks or months during which they had felt marked relief from their original troubles. Those who still enjoy improved nasal respiration without frontal pain often assume an independent asthmoidal bronchitis and are frequent clients of pulmonologists, consuming numerous symptomatic remedies before reconsideration of occult sinusitis as the cause of the spread of mucosal irritation.
Nasal endoscopy in such cases may convey the impression of recovered mucosa in the visible cavities; then CT imaging is indicated to detect foci in remote areas. Alternatively, the examiner may find minor changes, such as mucosal edema or small polyps. If such changes occlude a small maxillary window or the frontonasal duct (Fig. 8.1a, b) , reopening these as a minor intervention will help. Solitary scars bridging the anterior ethmoid Fig. 8.2) are apt to induce a vicious circle of congestion, reinfection, and polyposis. The worst case is reocclusion of the ethmoid by scarred, hyperplastic mucosa Fig. 8.3).
Progressive chronic sinusitis may have survived a previous surgical intervention for various reasons, including resistant microorganisms, a blockage of lymph drainage by scar formation, or necrotic bone remnants and sequestra Fig. 8.4). Obliteration of the anterior ethmoid by bridging collagen tissue will disturb ventilation and the self-cleansing mechanism of adjacent mucosal islands and also the reorganization of a lymphatic network, causing progression of hyperplastic mucositis into compartments that had until then been healthy. This not infrequently happens in the new outlet of the frontal sinus, and even in the edge of a widely open nasoantrostomy (Fig. 8.5a) . The same sequelae can result from granulations that may become prominent and epithelialized and can grow into the shape of large polyps (Fig. 8.5b) , occluding the nasofrontostomy. Chu et al. 1997 have analyzed revision cases and defined sites of predilection of persisting sinusitus; a similar report was given by Ramadan 1999.
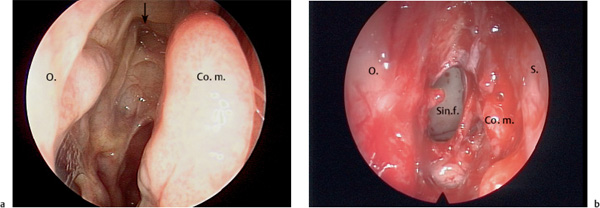
Fig. 8.1 a, b Reclosure of the nasofrontal duct by a thin fibromucosal scar (↓).
a At first glance, a healed ethmoid 6 months after pansinus operation in a patient suffering from frontal headache.
b Reopened and widened frontoethmoidal window draining a frontal empyema.
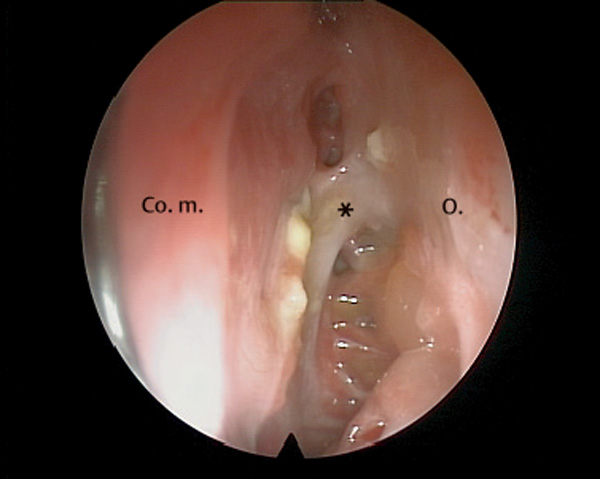
Fig. 8.2 A small, fresh scar (*) bridging the most anterior ethmoid occludes the nasofrontal duct.
Another cardinal problem is laterofi xation of a trimmed middle turbinate. After partial turbinetcomy with exenteration of polypous turbinal cells, the sagittal ground lamella loses its stability and tends to a lateral defl ection (Fig. 8.6a, b) , which also not infrequently results from splitting of a concha bullosa. Prophylaxis of laterofixation by a so-called synechia technique–fixation to the nasal septum (Bolger et al. 1999; Lindemann et al. 2002)– appears to be questionable with regard to an open olfactory rim.
Injury of the mucoperiosteum can induce appositional osteoneogenesis . This circumscribed but sometimes extensive growth of new bone is typical after radical surgery with generous sacrifice of the lining mucoperiosteum. It does not appear under the original mucoperiosteum. Its incidence is irregular, its pathogenesis unknown, reminiscent of similar reactions in middle ear surgery. Sites of predilection are the maxillary sinus and the sphenoid Fig. 8.7). When it occurs at the resected nasofrontal duct, severe stenosis follows, a reminder to preserve at least 50% of its mucosal lining.
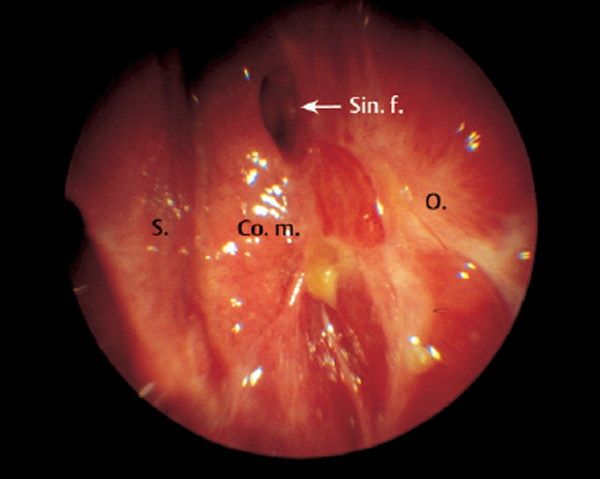
Fig. 8.3 Scarred left ethmoid with occluded remnant cells sustaining chronic rhinosinusitis.

Fig. 8.4 Bone fragment (*) left in the left maxillary sinus inducing granuloma with persistent mucositis (axial CT).
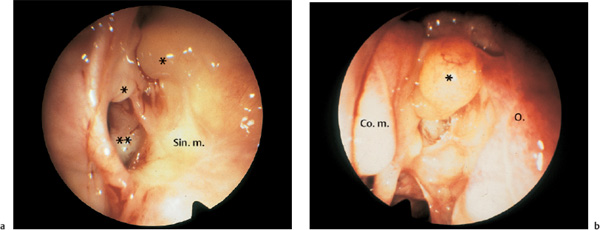
b Large granulation polyp (*) in the left anterior ethmoid blocking the nasofrontal duct after endoscopic ethmoidectomy and insufficient aftercare.
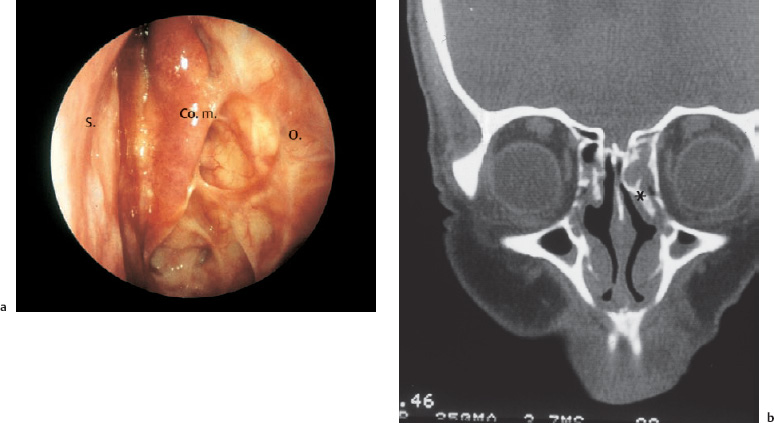
Fig. 8.6 a, b Laterofixation of the middle turbinate after endoscopic ethmoidectomy.
a Occlusion of the anterior ethmoids by the middle turbinate fixed to the lateral ethmoidal wall by scar formation (70° telescope).
b Coronal CT section showing laterofixation of the left middle turbinate (*) to the orbital wall and persistent ethmoiditis.
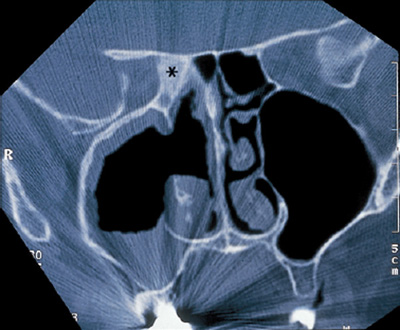
Fig. 8.7 Osteoneogenesis (*) of the right sphenoid bone from persistent unilateral pansinusitis after multiple endonasal and external pansinus operations with mutilating turbinectomies.
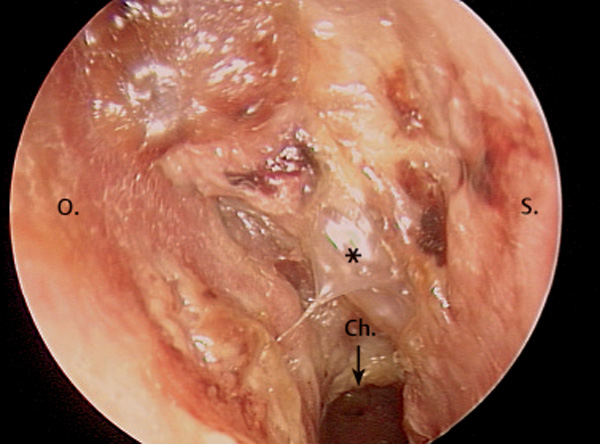
Fig. 8.8 Therapy-resistant secreting granulations (*) in a right ethmoid having destroyed the middle turbinate. Histological biopsy revealed Wegner granulomatosis (70° telescope).
Therapy-resistant persistence or recurrence of granulations or polyps, on the other hand, should alert the rhinologist to possible underlying systemic diseases such as mucoviscidosis, ASA intolerance Widal disease), ciliary dysfunction syndrome, and Wegener granulomatosis (Fig. 8.8). Even inverted papillomas may hide beneath unsuspicious polypoid hyperplasia.
Endoscopic examination of the nasal cavity and the paranasal surgical field will reveal any pathological secretion, mucosal swelling and polyps, and open communication of the operated sinuses with the nose. Even more informative is a new CT scan for the detection of diseased cells and cavities, regrowth of polyps, and reclosure of ducts and windows by granulations and scars. It will, in particular, reveal occluded compartments and mucoceles, which might eventually become pathological abnormalities of the bony structures. Additional to an endoscopic examination, a CT scan therefore appears prudent in order to trace the obliterated or stenotic bottlenecks where ventilation and drainage are hampered. In all such cases, especially when progressive nasal polyposis is blocking the functional anatomy Fig. 8.9), one should not hesitate to propose another pansinus operation with concomitant application of steroids.
Laboratory investigations will include swabs for the detection of problematic germs or mycosis and perhaps testing for an allergic syndrome if this has not been done before. A biopsy for histological examination will differentiate serious abnormalities. Also a general check-up for the exclusion of diabetes, blood disease and renal disease, or other systemic deficits is appropriate, as is inquiry about constant intake of drugs relevant to the mucosa, e. g., antihypertensives or anticonvulsives, and about environmental factors (see below).
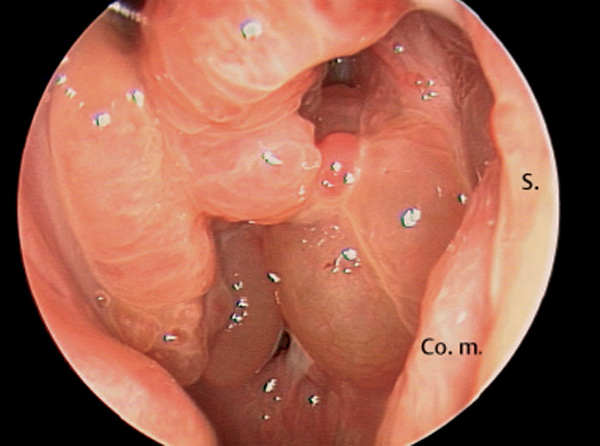
Fig. 8.9 Massive recurrent polyposis after pansinus operation obliterating the ethmoids and occluding the outlets of the paranasal cavities.
Revision procedures for persistent or recurrent sinusitis after previous endonasal sinus operations are basically performed through a further endonasal endoscopic approach. This was reccommended as a “second-look procedure” after pediatric FESS (Walner et al. 1998). Even a second or third repeat can be carried out with this access. I do not see any necessity to switch to an external approach if the initial intervention did not destroy the bony superstructure by a transfacial or transoral ouverture. However, even in this situation, which today is rare, a strictly endoscopic repair may occasionally be feasible. The main concern with any kind of approach is the completion or reorganization of a thorough passage of air and secretions through the whole pneumatization, with utmost effort to preserve the residual mucosa. For this purpose the revision will concentrate on the areas causing blockage. The second attempt thus aims at the repositioning and trimming of deflected turbinates, possibly at a revision septoplasty, and also at the removal of the most prominent polyps, and finally at the remodeling of involved windows and tunnels. Such revisions are beneficial in about 80% of cases and had to be repeated in the rest. Recourse to radical mucosectomy with total exenteration of the diseased compartments, as recommended by schools (Kerrebijn et al. 1996, Videler et al. 2006), appears obsolete and was not practiced by the author. Endoscopic procedures for revisional sinus surgery were also postulated by May et al. 1994, Duncavage 1995, and Parsons et al. 1996, who gave hints for mastering difficult situations. Other authors also consider external approaches as justifi ed options for problematic repeat surgery (Kerrebijn et al. 1996; Moses et al. 1998; Klossek 2000; Rouvier and Peynegre 2000; Videler et al. 2006).
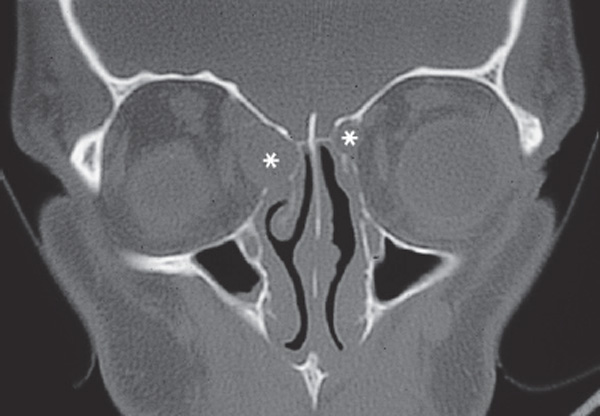

Fig. 8.11 Erosion of the sphenoid bone from a large mucopyocele (*) in a case of polypous pansinusitis (coronal CT).
It is advisable to implement the steps described above systematically: that is, the examination and reformation of the middle turbinate, which is often lateralized by scar bridges to the outer wall, thus occluding the ethmoids (see Fig. 8.6a, b) . Behind such a barrier a mucocele may develop into the orbit Fig. 8.10). Then follows the examination of the posterior ethmoid and the sphenoid sinus; inspection of the ethmoid roof posteroanteriorly along the now visible base of the skull; reexposure of the most anterior part of the ethmoid region as far as the opening of the frontal sinus with removal of granulations, scars, or polyps (see Fig. 8.5b) ; and revision of the antrostomy. A higher complication rate (9.9%) in ESS revisions due to scar formation and distorted anatomy was reported by Jiang and Hsu (2002). Navigational aids may serve as a valuable adjunct (Chiu and Vaughan 2004).
The posterior ethmoid and the sphenoid cavity usually pose minor problems. The endoscopic revision will scrutinize the cell system and ensure free communication between ethmoid and sphenoid with free passage also to the nasal meatus. Particular attention must be paid to the lateral sphenoid wall in which the internal carotid artery and the optic nerve may have been denuded by a persistent polyposis and now be endangered by the repeat sphenoidotomy Fig. 8.11).
Narrow passages are most frequently involved with reclosure: The most critical isthmus is the transition between anterior ethmoid and the frontal sinus. One will often find one or more cells which were not opened with the previous ethmoidectomy, either having been overlooked then or appearing healthy at that time. The frontoethmoidal tunnel is reopened by grasping fresh polyposis and punching bridging scars. The Nd:YAG laser has proved useful for bloodless excision of scar tissue at this critical place. Its application, however, will injure the adjacent mucosa, which has to be considered during the postoperative aftercare. If possible, the bony nasofrontostomy should be enlarged to a diameter of at least 5 mm, which is achieved with the help of a sharp curette or a diamond rasp. On rare occasions a new, broader nasofrontostomy has to be established using the technique described in Chapter 6, eventually utilizing the transseptal resections of the frontal sinus floor and with a median drainage of both frontal sinuses according to Draf III. Another frequent problem is the reclosure of the maxillary sinus. Infraturbinal windows often obliterate by impression of the inferior turbinate with its subsequent fibrous adhesion. The turbinate then has to be retracted and trimmed, and the adhesions excised. Additional installation of a supraturbinal antrostomy would be appropriate. The endoscopic reopening of a closed antrostomy in the middle nasal meatus follows the standard recipe. If possible, a flap of antral mucosa is mobilized and swung into the window in order to enhance the mucociliary transport from the cavity into the nose (see eversion technique on p. 127).
Polyps and edematous cystlike protrusions of the lining mucosa, often present even with an open nasoantrostomy, can simply be the result of a disturbed mucociliary transport through the window (see Fig. 8.5a) . They are resected with sharp forceps only if they are pedicled. If broadly based they are left in position and subjected to conservative aftercare. The precise pathophysiology inducing recurrent polypoid edemas remains obscure (Rouvier and Peynegre 2000).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


