10 Facial Trauma
Trauma Evaluation
1 | What is the first step in treating every trauma patient? | Ensure the patient has a safe and adequate airway (airway, breathing, circulation, or ABCs) |
2 | List the contraindications to cricothyrotomy. | Contraindicatioins include cricotracheal separation, laryngeal fracture, and young age. Children younger than 5 to 12 years of age should have needle cricothyrotomy or primary tracheostomy because of anatomical differences. |
3 | Describe the Glasgow Coma Scale (GCS) score scoring system. ( | The GCS maximum score is 15, and the minimum score is 3. The GCS is based on the cumulative score from three categories: eye opening, verbal responses, and motor responses. |
Behavior | Best Response | Score |
Eye opening | Spontaneous | 4 |
| To verbal command | 3 |
| To pain | 2 |
| None | 1 |
Verbal response | Oriented | 5 |
| Confused, but coherent speech | 4 |
| Inappropriate words | 3 |
| Incomprehensible sounds | 2 |
| No sounds | 1 |
Motor response | Obeys commands | 6 |
| Purposeful movement | 5 |
| Withdraws in response | 4 |
| Flexion in response to pain (decorticate posturing) | 3 |
| Extension in response to pain (decerebrate posturing) | 2 |
| No response | 1 |
Data from Teasdale G, Jennet B. Assessment of coma and impaired consciousness: a practical scale. Lancet. 1974 Jul 13;2 (7872):81–84. | ||
4 | What measure is a good indicator of the resuscitation status of a trauma patient with significant blood loss? | Urine output |
5 | Based on the physiology of a 70-kg man, roughly how much blood loss must occur before hypotension results? | 1.5 to 2 L |
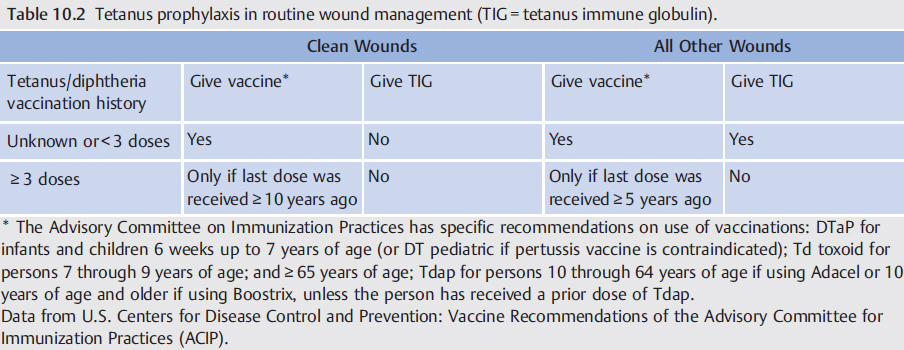
In an adult patient who is unsure of his or her vaccination history, what tetanus prophylaxis should be provided after a deep cut to the hand with a rusty knife? ( | Tetanus-diphtheria and tetanus immune globulin |
7 | What radiographic examination is most helpful in evaluating maxillofacial trauma? | Dedicated axial, sagittal, and coronal maxillofacial computed tomography (CT) with fine cuts (1 to 3 mm), including bone and soft tissue windows. Head and neck CT should also be obtained if there is concern for intracranial or neck/laryngeal injury. |
Soft Tissue Trauma
8 | List the bacteria commonly present in dog bites. | Pasteurella multocida, Staphylococcus aureus, Streptococcus viridans, and oral anaerobes |
9 | As a general rule, how long after initial injury can simple lacerations be closed? | Up to 3 days |
10 | What are the benefits of applying a negative pressure wound VAC to a partial avulsion injury? | Application of subatmospheric pressure has been shown to decrease bacterial counts, promote granulation tissue formation, and improve the rate of contracture. |
11 | Cleaning soft tissue injuries with hydrogen peroxide, modified Dakin’s solution, or povidoneiodine has been shown (in vitro) to be toxic to what cell types? | Fibroblasts and keratinocytes |
12 | Pigmented debris left in a wound bed may lead to what complication? | Traumatic tattooing |
13 | What is the mechanism of a pincushion (trapdoor) deformity after soft tissue trauma? | • When elevated or redundant tissue abuts a curvilinear-shaped scar • Most likely results from concentric wound contracture and lymphedema |
14 | Why should eyebrows be trimmed conservatively (not shaved) when treating patients with extensive facial trauma? | Regrowth of eyebrow hair may take as long as 6 months, and hair regrowth may be incomplete. |
15 | What suture technique is best for everting skin edges when closing a soft tissue laceration? | Vertical mattress |
16 | As a general rule, what suture type should be used to close the epidermis of young pediatric patients? | Absorbable suture is used because permanent suture will be difficult to remove in the office setting. |
Which wound adhesive is approved by the Food and Drug Administration (FDA) for closure of skin? | Octyl-2-cyanoacrylate (Dermabond) | |
18 | What is the mechanism of action of the tissue adhesive octyl-2-cyanoacrylate? | On exposure to moisture, octyl-2-cyanoacrylate undergoes an exothermic reaction as it polymerizes to form a strong tissue bond. |
19 | How does the location of a facial laceration influence whether or not wound exploration should be carried out for facial nerve neurorrhaphy? | Because of the extensive distal arborization of the facial nerve, injuries medial to the lateral canthus are unlikely to result in significant facial nerve deficits and generally do not warrant wound exploration. |
20 | What is the preferred management of a traumatically avulsed segment of the proximal extra-temporal facial nerve? | Mobilization with primary (end-to-end) neurorrhaphy is preferred. If a tension-free anastomosis cannot be obtained, then an interposition cable graft using greater auricular nerve or sural nerve should be used. |
21 | What treatment options can be used to decrease the risk of sialocele after traumatic parotid duct transection? | Options include primary anastomosis over a stent, duct ligation, or fistulization of the duct into the oral cavity. |
22 | What length of the lower lip can be managed with primary closure without significant distortion or microstomia? | Loss of up to one-third, or even one-half, of the lower lip can be managed with primary closure without significant distortion or resultant microstomia. |
23 | How much of the eyelid can be closed primarily after an avulsion injury? | 25% |
24 | What must be done to the avulsed segment of the auricle before its burial in a postauricular pocket for delayed reconstruction? | De-epithelialization of the avulsed segment |
25 | What antibiotic class should be used for injuries involving cartilage? | Fluoroquinolones should be used in adult and adolescent patients to adequately cover Pseudomonas aeruginosa. Fluoroquinolones represent the only oral antibiotic class with reliable activity against Pseudomonas spp. Parenteral anti-psuedomonal cephalosporins (ceftazidime and cefepime) should be used in children if perichondritis or chondritis is suspected. |
26 | What is the definition of a first-degree burn? | Damage no deeper than the epidermis, resulting in pain and erythema, but little or no permanent injury |
27 | What is the definition of a second-degree burn? | Injury involves the epidermis and a portion of the dermis (partial thickness) and is accompanied by pain, erythema, and blistering. The depth of dermal injury is used to further stratify second-degree burns as being either superficial or deep. |
28 | What is the definition of a third-degree burn? | Injury involves the epidermis and the full thickness of the dermis, destroying adnexal structures, blood vessels, and nerve endings. |
29 | The head and neck make up what percentage of the total body surface area (TBSA)? | 9% The “rule of nines” for calculating TBSA: • Each leg = 18% TBSA • Each arm = 9% TBSA • Anterior trunk = 18% TBSA • Posterior trunk = 18% TBSA • Head and neck = 9% TBSA |
30 | What is the Parkland formula for fluid resuscitation of burn victims? | Total volume is administered in the first 24 hours of resuscitation (with lactated Ringer’s solution) = 4 mL x weight (kg) x %TBSA burned. Half of the calculated volume is given over the first 8 hours, and the remaining volume is delivered at an even rate over the next 16 hours. |
In addition to IV antibiotics, why are topical antibiotics recommended to prevent superinfection in burn patients? | Burn eschar has a poor blood supply, decreasing the likelihood that therapeutic levels of systemically delivered antibiotic will penetrate the wound bed. | |
32 | When should burns involving the oral commissure be reconstructed? | Most surgeons recommend initial observation with conservative wound care and waiting to surgically intervene only after full scar maturation. |
33 | What treatment should be considered for patients with oral commissure electrical burns to decrease the risk of microstomia? | Oral appliance use is designed to splint the oral commissure. |
Neck, Larynx, and Trachea Trauma
34 | The Battle sign refers to what physical examination finding? | Postauricular ecchymosis that suggests a basilar skull fracture |
35 | After a head trauma, the patient experiences massive hemorrhage from the ear canal with postauricular ecchymosis. What is the next step in this patient’s treatment? | Pack the ear canal to control bleeding, and perform an arterial angiogram to examine for petrous carotid injury. |
36 | Subcutaneous emphysema that extends from the neck into the face travels in what plane? | Along the platysma and subcutaneous musculoaponeurotic system (SMAS) |
37 | Describe the anatomical boundaries of the three zones of the neck used for the evaluation and treatment of penetrating neck trauma. ( | • Zone I: Clavicle and sternal notch to cricoid cartilage • Zone II: Cricoid cartilage to angle of mandible • Zone III: Angle of mandible to skull base |
Fig. 10.1 Zones of the neck for evaluation of penetrating trauma. (Used with permission from Thieme Atlas of Anatomy: Head and Neuroanatomy, © Thieme 2007, illustration by Karl Wesker.)
With penetrating injuries to zone I of the neck, what structures are at risk of damage? | Aortic arch, carotid and vertebral arteries, subclavian vessels, innominate vessels, lung apices, esophagus, trachea, brachial plexus, recurrent laryngeal nerves, and thoracic duct are at risk. | |
39 | With penetrating injuries to zone II of the neck, what structures are at risk of damage? | Common carotid artery with both internal and external branches, phrenic nerve, vagus nerve, hypoglossal nerve, internal jugular vein, larynx, hypopharynx, and proximal esophagus are at risk. |
40 | With penetrating injuries to zone III of the neck, what structures are at risk of damage? | Distal internal carotid artery, external carotid artery with major branches, vertebral artery, jugular vein with contributing venous drainage (retromandibular, facial, etc.), prevertebral venous plexus, parotid gland, and facial nerve are at risk. |
41 | Of the neck zones, which is the most surgically accessible? | Zone II |
42 | Describe the main factors that influence the injury incurred from ballistic strike. | Kinetic energy (KE) (velocity is more important than mass), design of projectile, composition of receiving tissue KE = (½) (mass) (velocity)2 |
43 | What commonly used radiographic technique has been shown to reduce significantly the number of negative surgical neck explorations in penetrating neck trauma? | CT angiography |
44 | When performing esophagography in a patient with penetrating neck trauma, why is it important to use a water-soluble contrast agent? | Extravasation of barium into the mediastinum can cause mediastinitis and fibrosis. This risk is mitigated by the use of water-soluble contrast agents (Gastrografin). However, barium is less toxic to the lungs if it is aspirated. |
45 | In penetrating neck trauma, which structure, if it is not violated, significantly decreases the probability of aerodigestive or vascular injury? | Platysma |
46 | Review the signs of carotid vascular injury after penetrating neck trauma. | Hematoma/ecchymosis, hypovolemic shock, external hemorrhage, absent carotid pulse, carotid bruit or thrill, diminished ipsilateral radial pulse, contralateral hemiparesis, and altered mental status |
47 | Review the signs of aerodigestive injury in penetrating neck trauma. | Dysphagia, hoarseness, subcutaneous emphysema/crepitus, hemoptysis, hematemesis, gas escape from neck wound, dyspnea, airway obstruction, and stridor |
48 | What are the indications for immediate surgical exploration after penetrating neck injury? | An unstable patient with significant hemorrhage, expanding hematoma, nonexpanding hematoma with hemodynamic instability, hemomediastinum, hemothorax, airway decompensation |
49 | What are common findings in blunt laryngeal trauma? | Subcutaneous emphysema, dysphagia, dysphonia, dyspnea, stridor, hemoptysis, neck swelling |
50 | Describe the Schaefer classification system of laryngeal injury. | • Group I: Minor endolaryngeal hematoma without detectable fracture • Group II: Edema, hematoma, minor mucosal disruption without exposed cartilage, nondisplaced fractures • Group III: Massive edema, mucosal disruption, exposed cartilage, vocal fold immobility, displaced fracture • Group IV: Group III with two or more fracture lines or massive trauma to laryngeal mucosa • Group V: Complete laryngotracheal separation |
51 | List conservative therapies that should be considered when treating a patient with a laryngeal fracture. | Voice rest, humidified blow-by, steroids, antibiotics, anti-reflux medications |
Review the symptoms of laryngeal fracture. | Dysphonia, neck pain, odynophagia, dyspnea, dysphagia | |
53 | Review the signs of laryngeal fracture. | Hemoptysis, neck tenderness, subcutaneous emphysema, anterior neck ecchymosis, laryngeal deviation, loss of laryngeal prominence, stridor |
54 | What is the most important imaging study for evaluating laryngeal trauma? | Fine-cut CT |
55 | Which age group tends to have the highest mortality after laryngeal trauma? | Patients older than 70 years of age |
56 | Describe the reasons why children rarely sustain laryngeal fractures. | Their larynx is situated higher in the neck and is therefore more protected by the mandible; cartilages are not ossified and therefore are more resistant to fracture. |
57 | Describe the mechanism of injury for laryngeal fractures. | Compression of the larynx between an intrusive object and the rigid cervical spine The degree of injury depends on the amount of compressive force and degree of cartilage ossification. |
58 | What is the preferred method of airway management for patients with advanced laryngeal trauma? | Awake tracheotomy in the operating room |
59 | List the potential pitfalls and complications associated with endotracheal intubation in patients with laryngeal trauma. | Cervical spine injuries, laryngeal lacerations and hemorrhage, displaced laryngeal architecture, and cricotracheal separation |
60 | Describe the steps to repair advanced laryngeal fractures. | Secure the airway with awake tracheotomy, direct laryngoscopy with rigid bronchoscopy, neck exploration, laryngotracheal/endolaryngeal repair, cartilage stabilization |
61 | How long are stents usually left in place after laryngeal fracture repair? | In general, 2 to 3 weeks |
62 | During an open laryngeal repair, a keel is useful in preventing what type of complication? | Anterior glottic web |
Plating and Fixation
63 | What are the general treatment goals of facial reconstruction following trauma? | Restoration of form (facial height, facial width, and facial projection) and function (airway, occlusion, mastication) |
64 | What must fracture fixation accomplish to allow for direct (primary) bone healing? | Fixation must overcome natural forces acting across the fracture site that would lead to mechanical instability and poor apposition of the fractured segments. |
65 | Name the two major types of plating materials. | • Metal • Resorbable |
66 |



