18 Facial Plastic Surgery in Geriatric Patients
 Introduction
Introduction
Several predictable changes and alterations are typical and normal sequelae of the neck and facial aging process. Unlike other components of the body’s predictable aging changes, aging in the face and neck region carries other significant implications, including those that impact cultural, social, and personal perceptions. Historically there has been an evolution of facial rejuvenation procedures in response to those perceptions. The procedures have gained significant public acceptance and desirability. In the not too distant past facial procedures were often felt to be within the realm of wealthy celebrities or others in the entertainment business. Today these procedures are widely accepted and actively explored by a wide spectrum of social, economic, and ethnic backgrounds. The goal is to achieve an enhanced self-perception of greater fitness and youth coupled with a response to cultural pressures to maintain a youthful appearance related to work, economic, and various social interactions.1,2
Although the geriatric population requires facial plastic surgery for facial trauma and fractures, facial neoplasms, and occasionally persistent congenital defects, the focus of facial plastic surgery in the geriatric population more frequently addresses facial aging processes. An individual’s age is usually judged according to appearance of the skin.3 Although much attention is focused on cutaneous gerontology, the appearance of cutaneous senescence is actually based on a combination of skeletal structure, soft tissue, and skin (Fig. 18.1). The primary changes in a person’s three-dimensional skeletal contour contribute to secondary changes in the overlying soft tissue and skin. It has been said that a youthful face represents that period in time when a particular set of skeletal proportions are ideal for their soft tissue envelope.
What is generally termed facial aging is in reality a combination of the aforementioned factors. Facial wrinkles or rhytids are related to changes in the skin secondary to a variety of factors, including chronological skin aging, ultraviolet (UV) and other environmental factors leading to photoaging, hyperdynamic facial expressions, and skin folding secondary to loss of soft tissue support and skeletal changes. Reversal or techniques to counteract these changes create the foundation for facial plastic surgery in the geriatric patient (Fig. 18.2).
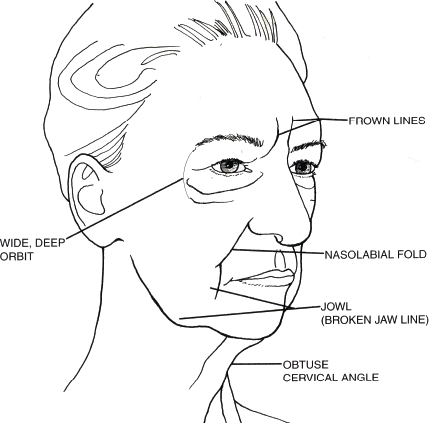
Fig. 18.1 Typical aging changes. (Used with permission from Facial Plast Surg Clin North Am 2001;9(2):179–187.)
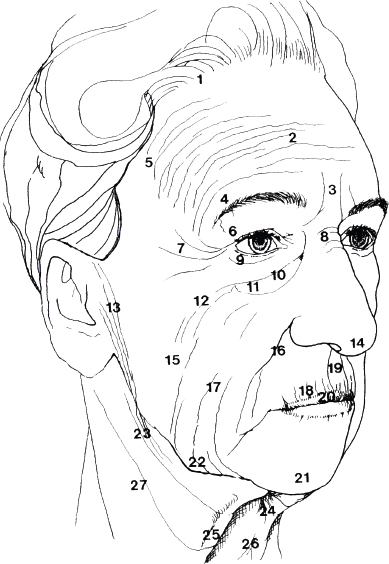
Fig. 18.2 Topographic geriatric facial changes. (Used with permission from Facial Plast Surg Clin North Am 2001;9(2): 179–187.)
 Analysis and Pathophysiology of Facial Aging
Analysis and Pathophysiology of Facial Aging
Geriatric skin changes are a product of two basic processes. First is chronological aging, sometimes referred to as intrinsic aging, the changes of which are primarily genetic. Second is environmental or extrinsic aging, particularly from such stressors as sun exposure or smoking. Skin changes often seen in the geriatric patient include dyschromia, roughness, and multiple rhytids followed by persistently deeper folds. Structurally this occurs due to dermal atrophy, decreased collagen, and loss of cutaneous fat coupled with loss of inherent elasticity and increased melanogenesis4
The structural changes in soft tissue already noted are variable but can be significant as part of the aging process, two major forces impact these changes. First is chronological aging of the skin related to intrinsic passage of time and second, photoaging related to chronic ultraviolet light exposure. Other components may impact this as well, such as smoking and certain dietetic aspects.5 The skin of geriatric patients shows declining changes with age, which ae further accelerated in UV exposed photoaged skin. Photoaging is responsible for many of the age-associated cosmetic concerns, including dispigmentation, laxity, changes of pores, telangiectasia, a leathery appearance, and wrinkling. Vascular changes increase during this period, creating the tendency for bruising during activities of daily life as well as medical procedures. Loss as well as shifting and redistribution of subcutaneous tissue further contribute to folds and drooping skin. Because of these changes, dealing with soft tissue in the geriatric patient carries additional considerations as compared with more youthful patients:
• Cell replacement
• Immune response
• Injury response
• Barrier function
• Sensory perception
• Sweat production
• Sebum production
• Vitamin D production
The facial changes typically associated with the geriatric patient are a result of a combination of forces related to facial aging including gravity, soft tissue maturation, skeletal remodeling, facial muscular changes, and solar changes to the skin. The aging process comprises a complex and diverse set of elements, each of which leaves a specific and distinctive result on the aging face. The anatomical and tissue changes already noted are intimately interconnected, each having an impact on the other components. Skin, soft tissue, muscle, and skeleton, although affected individually by the aging process, present themselves as an interactive aging process acting in concert to result in the facial appearance typically seen in the geriatric patient.
 Geriatric Skin Changes
Geriatric Skin Changes
The geriatric patient displays several predictable changes related to ongoing aging affect. These changes include secondary results of gravity acting on skin that is becoming progressively thinner, dryer, and less elastic. There are genetic factors also influencing the location of facial wrinkles, and these progress as a result of cutaneous senescence combined with cumulative environmental insults.
Chronic solar exposure and UV interaction constitute the major environmental component contributing to the clinical changes that are typical of aging skin. This is accurately termed photoaging and is distinct from intrinsic or chronological aging.
The relationship of inherent aging changes in the geriatric patient’s skin can be contrasted with those changes that are compounded by photoaging and chronic solar exposure. More photologic changes and sun-protected skin consist primarily of fine wrinkling and laxity with occasional benign neoplasm development. Those who leave their skin exposed to chronic solar damage demonstrate changes of texture, color, and functional capacity. Color changes include dyschromia, often a yellow pallor, lentigines, and the gradual appearance of telangiectasia. Textural changes likewise accompany these variations and include a loss of palpable smoothness, keratosis, and increasing rhytids ending in persistent deep folds and creases. Histological changes associated with aging skin begin with a thinning of the viable epidermis and flattening of the dermal–epidermal junction. This is in contrast to photoaged skin in which the epidermis becomes increasingly thicker with a flattening of the dermal–epidermal junction.
Of the dermal structural elements, elastic fibers are prominently affected by the sequelae of both chronologically damaged and photodamaged skin. Chronically aged skin reveals elastic fibers that are slightly increased in thickness. Photodamaged skin shows striking histological changes with the presence of massive quantities of thickened bundles of degraded elastic fibers or dermal elastosis. The result of these various histological reactions and changes in aging skin is that the skin itself is less stretchable and less resilient. The loss of inheritant elasticity results in skin that is more lax with dependent draping that is prone to wrinkling from gravitational effects. There is also an increase in mechanical fragility and a susceptibility to lateral sheer stress combined with an increase in dryness and skin irritability.6
 Geriatric Facial Musculature
Geriatric Facial Musculature
Contractions and sphincteric actions of the facial musculature are responsible for facial expressions exhibiting emotion as well as functional actions including eye closing, lip movement, and numerous others. However, over time and combined with aging skin changes facial rhytids and folds are accentuated by this normal muscular action and begin to contribute to changes in facial appearance associated with aging in the geriatric patient. For example, continued contraction of the orbicularis component of the orbicularis oculi creates concentric folds emanating from the lateral canthus resulting in lines referred to as crow’s feet. The corrugator supercilii lies deep to the frontalis muscle and has it origin on the frontal bone medial to the eyebrows near the superior medial orbital rim. The corrugator acts as a brow abductor drawing the brows inferiorly and medially and thus ultimately producing vertical frown lines. In the same anatomical region, the procerus muscle originates on the lower part of the nasal bone and inserts in the skin overlying the nasion. This likewise pulls the medial brow inferiorly, creating transverse wrinkles over the nasal bridge. The antagonist of the brow depressors is the frontalis muscle, which is ultimately responsible for horizontal forehead creases. All of these actions, which are normal facial movements, ultimately contribute to an aging facial appearance and are key areas addressed, particularly by Botox (Allergan, Irvine, CA), as a treatment modality. Similarly, the normal muscle actions of the lower facial mimetic muscles and the perioral muscles all contribute to rhytids and skin folds related to aging changes in the lower face. Although it is a normal process for these hyperdynamic facial lines, crow’s feet, and glabellar furrows to reflect underlined muscular anatomy, the ultimate result is reflective of what are typically thought of as unaesthetic changes in the face related to aging.
 The Aging Nose
The Aging Nose
Often overlooked in terms of facial anatomical changes that are recognized as aging in the face are the progressive changes to nasal appearance and its impact on facial aesthetics. The nose at a central location is a key component of facial aesthetics and facial relationships, and the aging changes that affect the nose affect the rest of the facial appearance. Aging alters the nasal skeleton, cartilaginous framework, and soft tissue covering.7 Progressive descent of the nasal tip is often associated with loss of support from changes and attachment of the upper and lower level cartilages, which then lengthen and weaken the nasal tip support, thus lengthening and enlarging the nose. The nasal labia angle becomes increasingly acute in relationship to this loss of tip structure. The relative appearance of a nasal dorsal hump is exaggerated as the tip decreases in its projection. Pyriform remodeling affects the alar base, and, in combination with upper maxillary resorption, it results in superior repositioning and thus further narrowing of the nasal labial angle and accentuation of the tip ptosis. Chin pad ptosis secondary to bony resorption further contributes to the illusion of increased nasal length (Fig. 18.3).
Rhinoplasty of the geriatric patient often not only contributes to a more youthful appearance based on repositioning of the nasal anatomy but also frequently contributes to airway improvement. Aging changes to the nose that impact nasal function include loss of the internal nasal valve support, external valve collapse, and changes of narrow airway openings related to loss of tip support. Rhinoplasty is a frequent requirement in the aging patient because of these functional and airway difficulties in addition to aesthetic goals of attaining greater youthfulness and enhanced aesthetic facial appearance in the geriatric patient.
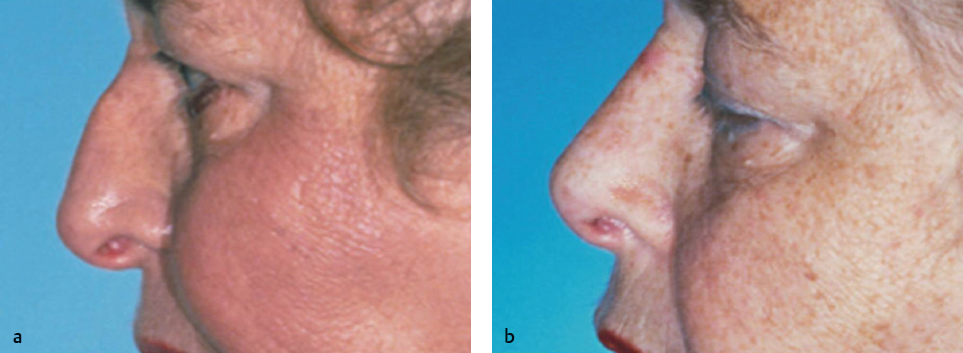
Fig. 18.3 (a) Typical findings in the geriatric nose include soft tissue thickening, loss of tip support, and narrowing of the nasolabial angle. (b) Postoperative improvements following rhinoplasty in the geriatric patient.
 Eyebrows and Eyelids in the Geriatric Patient
Eyebrows and Eyelids in the Geriatric Patient
The combination of gravity, loss of tissue elasticity, a loss of subcutaneous tissue, and at times bony resorption lead to inferior displacement of the brow. With aging, typically the eyebrow position descends from above the supraorbital rim to point of some portion below it. This contributes to excess accumulation of upper lid skin that accentuates ongoing skin changes of dermatochalasis with loss of eyelid creases and additional folds of skin over the upper lid. Excess sliding of skin and a weakened orbital septum allow interorbital fat to herniate, creating eyelid bags and protruding adipose tissue. The periorbital soft tissue in the more youthful patient is often shallow and described as an unbroken convex line from the lower eyelid to the cheek. With progressive aging those relationships change the dimensions and become wider and deeper as time progresses. Ptotic cheek fat may descend inferiorly, contributing to a melolabial fold leaving a cheek depression that can be accentuated by buccal fat attenuation. The orbicularis muscle becomes increasingly ptotic; with aging its inferior border becomes increasingly apparent. This creates the malar decent of the zygomatic eminence laterally resulting in deepening of the nasojugal fold, which continues to deepen with aging. Multiple surgical procedures in the aging patient are designed to correct and reverse these predictable changes. Procedures used individually or in combination include upper and lower blepharoplasty, brow lift, and forehead lift. These surgical procedures may be used independently or in combination with other facial aesthetic procedures depending on the severity of the aging changes in the geriatric patient as well as the patient’s aesthetic goals.
 Jowl and Neck in the Aging Patient
Jowl and Neck in the Aging Patient
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


