9 Facial Plastic and Reconstructive Surgery
Wound Healing and Scar Revision
1 | What are the layers of the skin from superficial to deep? | • Epidermis • Basement membrane • Dermis (papillary and reticular) • Subcutis |
2 | What are the layers of the epidermis from superficial to deep? | • Stratum corneum • Stratum lucidum • Stratum granulosum • Stratum spinosum • Stratum basale |
3 | What are epidermal appendages? | Skin-associated structures including hair follicles, apocrine glands, sebaceous glands, and eccrine (sweat) glands |
4 | What is the predominant type of collagen in the basement membrane? | Type IV collagen |
5 | What are the three phases of wound healing? ( | Inflammation, proliferation, and remodeling. Some authors also include hemostasis as the first phase. |
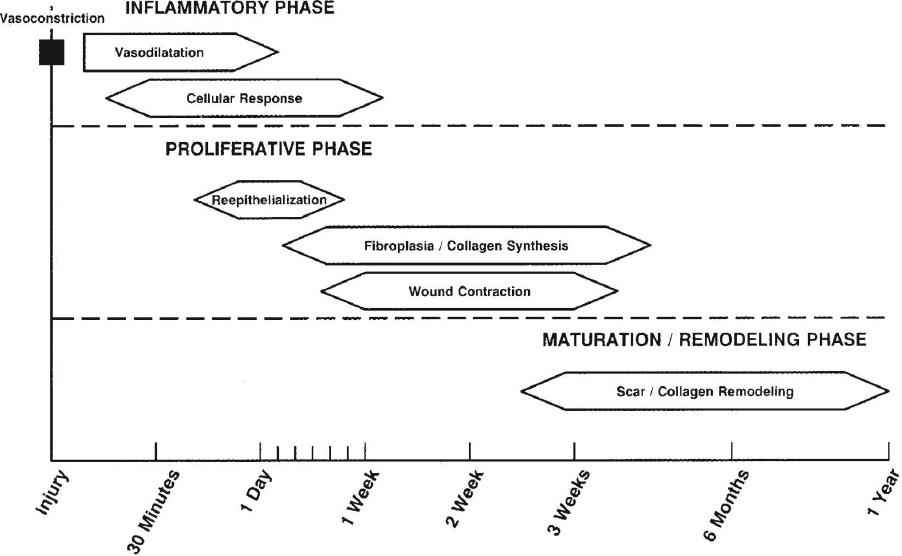
Fig. 9.1 The phases of wound healing. (Used with permission from Papel ID, Frodel J, Holt GR, et al, eds. Facial Plastic and Reconstructive Surgery 3rd Edition. New York, NY: Thieme; 2009.)
6 | What are four general categories of wound healing? | • Healing by primary intention: Two wound edges are brought together as the primary intention of the surgeon. • Delayed primary healing: Two wound edges are not brought together immediately but are reapproximated and closed at a later time. • Epithelialization Occurs in partial-thickness wounds as epithelial cells migrate and replicate over the wound. |
7 | What cell types are primarily involved in the inflammatory phase? | After vasoconstriction and subsequent vasodilation, polymorphonuclear neutrophils arrive and predominate for the first 24 to 48 hours after injury. Following this, monocyte migration occurs. |
8 | What cell type synthesizes collagen? | Fibroblasts |
9 | What cell type is responsible for wound contraction during healing? | Myofibroblasts containing microfilaments capable of producing contractile forces. These cells predominate the fibroblast population during the second week of wound healing. |
10 | What major events occur during the proliferative phase of wound healing? | Re-epithelialization, neovascularization, collagen deposition, and wound contraction |
11 | During which phase of healing are keratinocytes, fibroblasts, and endothelial cells recruited to the wound? | Proliferative phase |
12 | During the proliferative phase, which cytokine modulates angiogenesis and neovascularization? | Vascular endothelial growth factor (VEGF) |
13 | How does hyperbaric oxygen therapy encourage wound healing? | It promotes angiogenesis, fibroblast proliferation, leukocyte activity, and is synergistic with antibiotic therapy. |
14 | What is the predominant type of collagen in an early scar? | Type III collagen |
15 | What is the approximate tensile strength of a healing wound at 3 months? | 50% of normal tissue |
16 | When is the remodeling phase of wound healing usually complete? | 12 months |
17 | What are the tenets of Halsted? | • Gentle handling of tissues • Aseptic technique • Sharp anatomical dissection of tissues • Careful hemostasis, using fine, nonirritating suture materials in minimal amounts • The obliteration of dead space in the wound • Avoidance of tension |
18 | How can local tissue factors impact wound healing? | Wound healing is compromised by any tissue effect that decreases oxygenation, increases infection risk, prolongs inflammation, delays neovascularization, or otherwise alters the normal process of healing. Examples include local infection, ischemia resulting from pressure necrosis (e.g., diabetic neuropathy, hematoma), alteration in tissue structure resulting from radiation therapy, locally destructive processes (neoplasia, wound desiccation). |
19 | What patients should be counseled about increased risk for postoperative infection or wound breakdown? | Patients with medical comorbidities, medications, or history of recent treatments, which alter the normal healing process or suppress the immune system. For example, patients who have undergone chemotherapy and radiation therapy, are taking immunosuppressants, or have diseases that affect the vasculature (e.g., peripheral vascular disease, diabetes, tobacco dependence.) are at increased risk for wound complications. |
What are relaxed skin tension lines? | They are the lines of minimal tension on the skin. They run parallel to natural wrinkle lines and are usually perpendicular to the force of action of the underlying muscles of facial expression. | |
21 | What are some of the technique- and patient-related factors that may lead to an aesthetically unacceptable scar? | • Patient variables: Diabetes, chronic steroid use, systemic vasculitis, vitamin deficiency, poor overall nutrition, chronic renal disease, wound infection, collagen vascular disease, sun exposure • Technical variables: Failure to clean the wound adequately, excessive tension on epidermal sutures, step-off between wound edges, rough handling of tissue, prolonged suture retention, failure to orient incision parallel to relaxed skin tension lines, delayed wound closure |
22 | What are some of the performance differences between monofilament and braided suture? | Monofilament suture has “memory” and usually requires more knots to secure a tie. Braided suture has more tensile strength but creates more resistance through tissue, induces a stronger inflammatory response, and is more likely to serve as a reservoir for microorganisms. |
23 | What type of surface contour is most favorable for wound healing by secondary intention? ( | Concave surfaces |
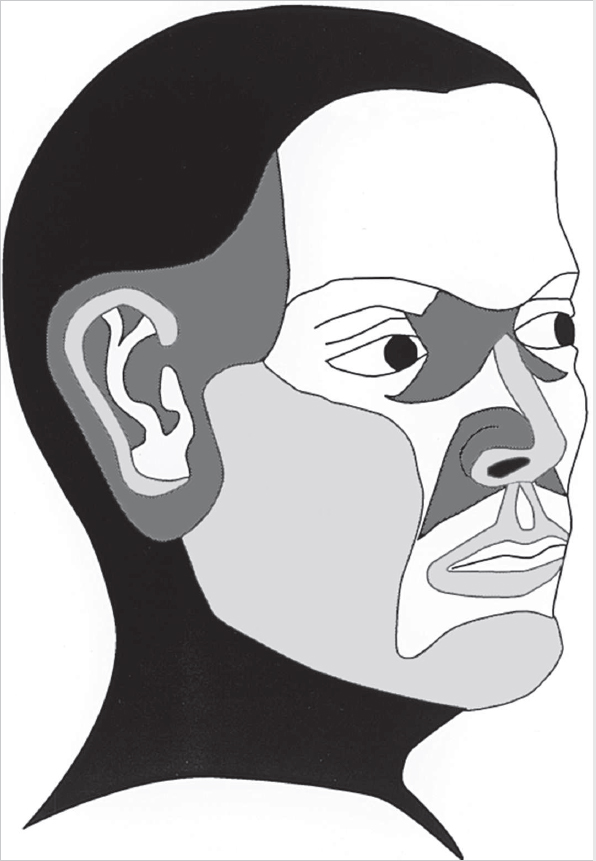
Fig. 9.2 Cosmetic results after wound healing by secondary intentention. Dark gray (concave surfaces of the nose, eye, ear, and temple) are usually associated with excellent results. White (forehead, antihelix, eyelids, rest of nose, lips, and cheeks) grant satisfactory results. Light gray (convex surfaces of the nose, lips, cheeks, chin and helix) provide variable results. (Used with permission from Papel ID, Frodel J, Holt GR, et al, eds. Facial Plastic and Reconstructive Surgery 3rd Edition. New York, NY: Thieme; 2009.)
What are some surgical options for scar revision? | Excision and closure with straight line, broken geometric line, W-plasty, Z-plasty, or local flap; excision and placement of a skin graft | |
25 | What medications may be injected into a scar to improve its appearance? | Steroids (triamcinolone diacetate), antimitotic agents (5-FU and bleomycin) |
26 | What is the role of silicone in scar revision? | The mechanism by which silicone sheeting reduces the appearance of hypertrophic scars has not been clearly elucidated. One hypothesis is that direct pressure exerted by silicone sheeting on the wound decreases scar hypertrophy. Another theory is that silicone’s ability to maintain a hydrated environment inhibits fibroblast production of collagen and glycosaminoglycans. |
27 | What is the primary difference between keloid formation and hypertrophic scarring? | Keloids spread beyond the boundaries of the original scar, whereas hypertrophic scars do not extend outside the wound perimeter. |
28 | Review some treatment options for keloids and hypertrophic scars. | Occlusive dressings, intralesional steroid injections, cryotherapy, radiation therapy, 5-FU, BOTOX injection, tacrolimus, retinoic acid, laser therapy, re-excision combined with above treatments |
Resurfacing
29 | What is dermabrasion, and what is its role in scar revision? | Dermabrasion is a mechanical method of removing the epidermis and creating a papillary to upper reticular dermal wound. Injuries to the epidermis and papillary dermis heal without scarring. Dermabrasion changes the depth of the scar to help it blend with surrounding normal tissue. It also seeks to create a wound with texture and color closely matching normal skin. |
30 | What layer of the dermis contains the predominant blood supply of the skin? | Reticular dermis |
31 | Dermabrasion injury to the papillary dermis results in production of what tissue elements? | Type I procollagen Type III procollagen Transforming growth factor-β1 |
32 | Routine prophylaxis for what infection is typically offered to patients before they undergo dermabrasion? | Herpes simplex virus, typically beginning 24 hours preoperatively and continuing for 5 days |
33 | Which Fitzpatrick skin types have the greatest risk of pigmentary dyschromia (hyper-pigmentation or hypopigmentation) after resurfacing? | Fitzpatrick type III through VI |
34 | What is the mechanism of action of hydroquinone? | Hydroquinone blocks tyrosinase from developing melanin precursors, thereby impeding new pigment formation as the new epidermis heals after a chemical peel. |
35 | What are the major indications for a medium depth chemical peel? | • Destruction of epidermal lesions • Resurfacing of moderate photoaging skin • Correction of pigmentary dyschromias • Repair of mild acne scars • Blending of photoaging skin with laser resurfacing |
36 | Baker-Gordon phenol is used to achieve what level of chemical peeling? | Deep chemical peel |
37 | What toxicities are associated with phenol chemical peels? | • Cardiotoxicity • Hepatotoxicity • Nephrotoxicity |
What methods may be used to limit the potential toxic effects of a phenol chemical peel? | • Administering intravenous hydration before and during the procedure • Increasing the duration of application • Electrocardiographic monitoring • Oxygen administration • Screening for patients with arrhythmias or hepatic/renal compromise or patients taking medications that may increase the risk of cardiac arrhythmias | |
39 | What does the acronym LASER stand for? | Light amplification by stimulated emission of radiation |
40 | What is the role of lasers in scar revision? | Lasers create thermal injury leading to collagen retraction. They can also be used for skin resurfacing to correct pigmentary defects. |
41 | What is the role of pulsed dye laser in scar revision? | A 585-nm wavelength pulse dyed laser can decrease the vascularity of scar tissue and reduce scar redness. The laser may also decrease the number and activity of fibroblasts. |
42 | What is the wavelength of the CO2 laser? ( | 10,600 nm, infrared spectrum |
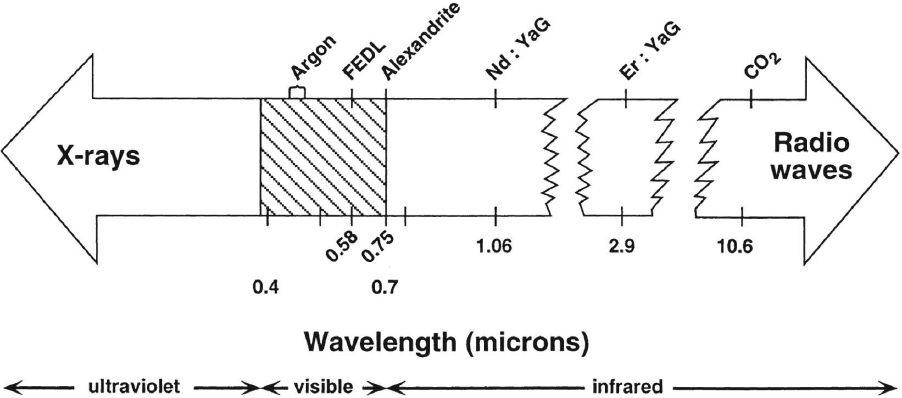
Fig. 9.3 The electromagnetic spectrum of surgical lasers. (Used with permission from Papel ID, Frodel J, Holt GR, et al, eds. Facial Plastic and Reconstructive Surgery 3rd Edition. New York, NY: Thieme; 2009.)
43 | What characteristic of CO2 lasers allows them to vaporize superficially and provide, for the most part, a what-you-see-is-what-you-get type of tissue interaction, similar to electrocautery? | They have increased absorption by tissues with high water content. |
44 | What is the primary chromophore for both the CO2 and Er:YAG laser? | Water. Er:YAG has strong tissue water absorption, approximately 12 times that of the CO2 laser. |
45 | What is the wavelength of the Er:YAG laser? | 2940 nm, infrared spectrum |
46 | What is the definition of laser fluency? | The amount of energy (joules) that is applied to the surface area of tissue (centimeters squared), expressed as J/cm2 |
The effect of a laser on specific tissue depends on what four factors? | • Laser wavelength • Laser energy density • Pulse duration • Tissue absorption | |
48 | How is laser power density altered? | By changing the focal length of the lens or changing the working distance |
49 | How does the pulsed delivery of a laser allow a higher energy delivery with less thermal injury? | By using the heat sink effect of the adjacent tissue and blood flow during the interpulse intervals |
50 | What is the term used to describe the characteristic of a laser’s ability to have photons move in the same temporal and spatial phase? | Coherence |
51 | What terms describe the laser-tissue surface interaction? | Absorption, transmission, reflection, scatter |
Implants and Fillers
52 | Which botulinum neuromodulator serotype demonstrates the longest duration of effect? | Serotype A (90 to 120 days) |
53 | What is the mechanism of action of BOTOX? | BOTOX prevents presynaptic neurosecretory vesicles from docking/fusing with the nerve synapse plasma membrane (degrades the SNAP-25 protein) and releasing acetylcholine into the neuromuscular junction. |
54 | Vertical glabellar furrows are most likely caused by which muscle? | Corrugator supercilii |
55 | What muscle arises in the medial end of the orbit/nasal prominence and interdigitates with the orbicularis oculi muscle laterally and the frontalis muscle superiorly? | Corrugator supercilii |
56 | What medication can be given to patients who develop botulinum toxin-related blepharoptosis, and what is its mechanism of action? | • Apraclonidine eye drops. An α2-adrenergic agonist, which causes Müller muscle to contract. • Phenylephrine can be used when apraclonidine is not available. |
57 | A patient does not appear to have further benefit after repeated botulinum toxin injections. What is the most likely cause? | Formation of neutralizing antibodies rendering resistance to the paralytic effect of the toxin. Often responds to switching to an alternate type. |
58 | What muscle may be treated with botulinum toxin to decrease the “peau d’orange” or dimpled chin appearance with facial animation? | The mentalis muscle |
59 | What is the role of fillers in scar revision? | To provide bulk to bring a depressed scar level with surrounding normal skin |
60 | List examples of tissue-derived injectable fillers? | • Bovine collagen (Zyderm, Zyplast) • Human particulate “dermal matrix” (Cymetra) • Cultured autologous fibroblasts (Isologen) |
61 | List examples of implantable soft tissue fillers. | • Human acellular dermis (AlloDerm) • Porcine acellular dermis (Surgisis) |
62 | List examples of synthesized selective bioactive (resorbable) injectable fillers. | • Calcium hydroxyapatite particles (Radiesse) • Polylactic acid particles (Sculptra) |
63 | What is an example of an implantable synthetic polymer? | Expanded polytetrafluoroethylene (Gore-Tex) |
64 | Which implant particle size is not readily phagocytized by macrophages? | 20 to 60 μm. Particles smaller than this have been shown to precipitate a chronic inflammatory response, whereas larger particles cannot be easily phagocytized and therefore elicit minimal inflammatory reaction. |
What are the challenges associated with the use of polymethylmethacrylate? | The final phase of polymerization is associated with an exothermic reaction that can cause tissue injury. It can become loose with time despite immobilization. The need for implant removal is higher if in contact with nasal or frontal sinus tissue. | |
66 | What is the primary advantage of dermal fat grafts over free adipose grafts? | There is less resorption than with free adipose grafts, although even up to 70% of dermal fat grafts are resorbed. |
67 | Describe some uses of facial fat grafting in facial aesthetic surgery. | Lip augmentation, effacement of glabellar rhytids, tear trough deformity, and deep nasolabial folds; replacing volume in areas of facial fat atrophy and to fill in depressed scars |
68 | When using tissue expanders, as a general rule of thumb, how much larger should the surface area of the base of the expander be than the defect size? | 2.5 times |
69 | In the context of tissue expanders, what is mechanical creep? | Rapid collagen and elastin realignment and dispersion of interstitial fluid and ground substance during applied soft tissue stretch |
70 | Review some complications from use of tissue expanders. | Hematoma, infection, extrusion, migration, necrosis of overlying tissue, loss of hair, pain, erosion of underlying bone |
71 | Why are gold and platinum the current metals of choice for eyelid-loading surgery? | Chemically inert and relatively dense |
Brow and Forehead Lift
72 | What muscles of facial expression are responsible for the horizontal rhytides of the glabella? | Procerus |
73 | What two dissection planes are commonly used during brow lift surgery? | • Subgaleal • Subperiosteal |
74 | What nonsurgical technique can be used for browplasty? | Selectively paralyzing the temporal brow depressors (lateral orbicularis muscle) with BOTOX type A which then allows unopposed elevation of the frontalis muscle |
75 | List the various surgical techniques used for brow rejuvenation | Temporal lift; direct brow, midforehead, temporal extension of rhytidectomy incision; coronal, pretrichial/trichophytic, endoscopic |
76 | What anatomical structure lies between the intermediate temporal fascia and the deep temporal fascia? | Intermediate fat pad |
77 | What surgical brow rejuvenation techniques involve subcutaneous tissue dissection? | Midforehead and direct brow |
78 | What is the sentinel vein? | A zygomaticotemporal vessel encountered between the deep temporal fascia and the temporoparietal fascia during dissection in the temporal region during brow lift surgery. It has been shown to point to the frontal branch of the facial nerve as it courses through the temporoparietal fascia. |
79 | What is the Pitanguy line? | A line that runs from the lobule to the lateral canthus. This line crosses the zygoma roughly at the midpoint from the helical root to the lateral canthus and approximates the location of the frontal branch of the facial nerve. |
80 | What is the aesthetic ideal for brow position in a man? | Horizontal, resting on the superior orbital rim |
What is the aesthetic ideal for brow position in a woman? ( | The brow should arc above the orbital rim with its highest point centered over the lateral limbus. |
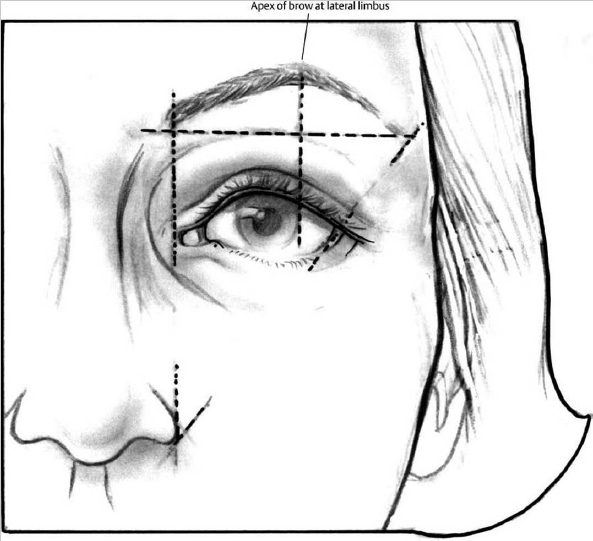
Fig. 9.4 The ideal female brow position rests just above the superior orbital rim with the apex tangent to the lateral limbus. (Used with permission from Papel ID, Frodel J, Holt GR, et al, eds. Facial Plastic and Reconstructive Surgery 3rd Edition. New York, NY: Thieme; 2009.)
82 | What incision placement strategy should be used during midforehead brow-lift surgery? | Centering incisions over existing rhytids and selecting two different vertical forehead creases to stagger the incisions |
83 | What brow-lift surgery technique is best used in a man with a receding hairline? | Midforehead |
84 | Currently, what is the surgical technique of choice for correction of both brow ptosis and forehead and glabellar rhytids? | Endoscopic blepharoplasty |
85 | What are contraindications to a coronal lift for brow ptosis? | • High female hairline • Male-pattern baldness • Brow asymmetries |
86 | In what percentage of patients will the supratrochlear or supraorbital nerves arise from a true foramen, putting them at risk for transection? | 10 to 30% |
87 | What muscle is considered the primary elevator of the brow? | Frontalis |
88 | The galea aponeurosis is contiguous with what two other anatomical structures? | The SMAS of the face below and the temporoparietal fascia (TPF) laterally. |
Ptosis and Blepharoplasty
89 | What are the four standard clinical measurements used for evaluating someone with ptosis? | • Palpebral fissure height • Marginal reflex distance • Upper eyelid crease distance • Levator excursion |
How does one assess eyelid ptosis? | Eyelid ptosis should be evaluated in primary gaze with the frontalis relaxed and the brow fixed. The average vertical palpebral fissure is approximately 10 mm. The levator function is tested by measuring the vertical excursion of the eyelid (normal 12 to 18 mm). The margin-to-reflex distance is the distance between the central corneal light reflex and the upper eyelid margin (normal ~ 4.5 mm). | |
91 | What is the normal position of the upper eyelid relative to the limbus? | The upper eyelid margin typically rests 1.5 mm below the superior corneal limbus, with the highest point just medial to the pupil. |
92 | Describe the ideal upper eyelid configuration. | The lid crease is 6 to 8 mm from the lash line in a man and 8 to 10 mm in a woman. The upper lid covers approximately 1.5 mm of the iris and does not reach the level of the pupil during primary gaze. |
93 | What two muscles are responsible for elevation of the upper eyelid? ( | Levator palpebrae superioris and Müller muscle |
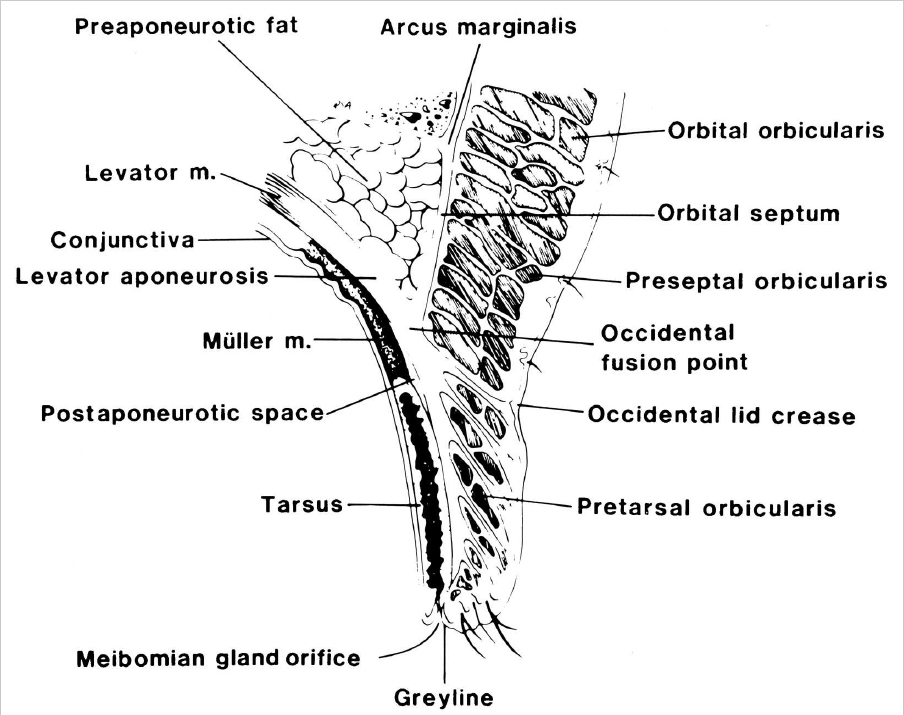
Fig. 9.5 Cross sectional anatomy of the upper eyelid demonstrating the position of the levator and Müller muscle. (Used with permission from Edelstein DR, ed. Revision Surgery in Otolaryngology. New York, NY: Thieme; 2009.)
94 | Where does the levator palpebrae superioris originate and insert? | It originates from the lesser wing of the sphenoid and inserts on the superior tarsal plate. |
What is the innervation of the levator palpebrae superioris? | The oculomotor nerve | |
96 | Where does Müller muscle originate and insert? | It originates from the undersurface of the levator palpebrae superioris and inserts on the superior aspect of the tarsus. |
97 | What is the innervation of Müller muscle? | Sympathetic nervous system from the superior cervical ganglion to the carotid plexus and along the oculomotor nerve |
98 | Describe the margin crease distance. | The distance from the upper eyelid crease to the upper eyelid margin measured during downgaze |
99 | Where should the inferior incision be placed during upper eyelid blepharoplasty? | At the natural lid crease, which is at the upper margin of the underlying superior tarsal plate (8 to 10 mm above the lid margin in women and 6 to 9 mm in men) |
100 | What are milia? | Milia are 1- to 2-mm cysts that appear as white, smooth nodules on the face. Histologically, they are identical to epidermoid cysts except for their smaller size. |
101 | Describe the marginal reflex distance-1? | Distance from the center of the pupillary light reflex to the upper eyelid margin during primary gaze |
102 | What is the marginal reflex distance-2? | The space between the lower eyelid margin and the pupillary light reflex during primary gaze (normally ~ 5 mm) |
103 | What is the difference between blepharoptosis and blepharochalasis? | • Blepharoptosis (ptosis) refers to an abnormally low-lying upper eyelid margin during primary gaze. • Blepharochalasis refers to a condition of unilateral or bilateral episodic painless, periorbital edema that leads to lid redundancy. |
104 | What is pseudoptosis? | When the upper eyelid appears to be low as a result of malposition of the globe or brow rather than eyelid dysfunction |
105 | What is the cause of an undesirable hollowed-out appearance after cosmetic blepharoplasty? | Excessive resection of orbital fat |
106 | What is the anatomical basis for the difference between the Asian and white upper eyelid? | In the Asian eyelid, the orbital septum fuses with the levator aponeurosis below the superior tarsal border. The accompanying preaponeurotic or orbital fat is allowed to proceed to the anterior tarsal surface, resulting in a full, thickened or puffy eyelid. In the white eyelid, the levator aponeurosis penetrates the orbital septum and orbicularis muscle attaching to the overlying dermis, creating a superior palpebral fold. |
107 | What is the primary risk of epicanthoplasty in the Asian patient? | Web formation in the medial canthal region |
108 | What percentage of Asians demonstrate a “single-eyelid,” and what percentage have an epicanthal fold? | 50% and 90%, respectively; the size of the fold is usually relatively small. |
109 | What is the most common form of ptosis? | Acquired aponeurotic or senile ptosis |
110 | What is a common clinical sign of acquired aponeurotic ptosis? | Normal or near normal levator function with an abnormally elevated upper eyelid crease |
111 | What is the most common type of congenital ptosis? | Congenital myogenic ptosis. Caused by dysgenesis of the levator palpebrae superioris in which the muscle fibers are replaced by fibroadipose tissue. |
112 | What percentage of congenital ptosis is unilateral? | Approximately 75% |
113 | What coexisting ocular condition is present in a significant number of patients with congenital ptosis? | Amblyopia |
Describe the phenylephrine test for evaluating ptosis? | This test involves placing dilute phenylepherine in the eye. After waiting 5 minutes, the palpebral fissure and marginal reflex distance are measured and compared with baseline. If there is a good response, then the Müller muscle conjunctival resection should be considered. If there was no response, the external levator advancement should be considered. | |
115 | Describe the clinical manifestation of myogenic ptosis secondary to myasthenia gravis. | Nearly all patients with myasthenia gravis develop ocular symptoms, including ptosis and diplopia. Ptosis is generally bilateral and worsens throughout the day. Symptoms may alternate from one eye to the other. |
116 | What surgical technique can be used for treatment of ptosis with poor or absent levator function? | Frontalis sling |
117 | What are the clinical manifestations of Marcus Gunn jaw-winking ptosis? | Elevation of a ptotic eyelid during ipsilateral activation of the mandibular division of the trigeminal nerve (chewing, jaw opening) |
Periocular Reconstruction
118 | What are the most common causes for needing eyelid reconstruction? | Eyelid tumor excision followed by trauma |
119 | What are the lamellae of the eyelid? | Anterior, middle, and posterior |
120 | What structures make up the anterior, middle and posterior lamellae of the eyelid? | • Anterior: Skin and orbicularis oculi • Middle: Orbital septum, orbital fat, and the suborbicularis fibroadipose tissue • Posterior: Eyelid retractors, tarsal plate, and conjunctiva |
121 | Describe the anatomy of the medial canthus? | The medial canthus consists of the lacrimal drainage system and the medial canthal tendon. The medial canthal tendon surrounds the lacrimal sac (creating a “pump”) and splits to form anterior and posterior heads attaching to the anterior and posterior lacrimal crests. The medical canthal tendon diverges to join the suspensory ligaments of the eyelid, the orbicularis oculi muscle, and the tarsal plate. |
122 | What types of defects of the upper eyelid can be allowed to heal by secondary intention with acceptable results? | Medial canthal region less than 1 cm and the upper eyelid when not involving the lid margin and less than 5 mm in diameter |
123 | What is the maximum defect size of an eyelid that can be closed primarily? | 25% in an adult and up to 45% in elderly patients with significant lid laxity |
124 | What is the most commonly used reconstructive option for a defect that involves more than 50% of the upper eyelid? | Cutler-Beard flap |
125 | After a Cutler-Beard flap reconstruction of the upper eyelid, what will the newly reconstructed eyelid lack? | Eyelashes and tarsus. Tarsus can be reconstructed if desired, but this is not typically done. |
126 | Describe a Tenzel rotation flap? | Semicircular musculocutaneous rotation flap that recruits redundant skin from the lateral orbit and can be used to reconstruct defects up to 60% of the width of the upper or lower eyelids |
127 | Lower eyelid defects of 50% or greater are most commonly reconstructed with what type of flap? | Hughes tarsoconjunctival flap |
128 | What anatomical layer of the eyelid does the Hughes tarsoconjunctival flap reconstruct? | Posterior lamella |
When are Hughes tarsoconjunctival flaps and Cutler-Beard flaps most commonly divided after initial surgery? |



