Facial Lacerations
Facial lacerations are common in children as a result of their frequent falls and accidents. The majority of these injuries are superficial and require minimal care. However, some of these lacerations have deeper and/or associated injuries that must be detected and treated.
36-1 Repair of Facial Lacerations
Indications
A facial laceration through the dermis that is too large to approximate with wound tape (such as Steri-Strips [3M]) or tissue adhesive (e.g., octylcyanoacrylate or butylcyanoacrylate) should be sutured. Wounds that are under significant tension or dynamic stress or are irregular require suture placement.
Preoperative Evaluation
The presence of any associated injury must be determined and appropriate trauma protocols should be followed to stabilize the patient first. Facial radiologic imaging is indicated if fractures are suspected.
Operative Technique
1. Lacerations should be anesthetized and cleansed of any foreign debris, and bleeding should be controlled.
2. Small lacerations that do not require deep tissue closure can be closed with wound tape or tissue adhesives. The tissue edges are approximated and held together with forceps or manual pressure as tape or adhesive is applied to the wound.
3. Small lacerations may be sutured using local anesthesia, but larger, complex lacerations of the head and neck are best closed utilizing sedation or even general anesthesia.
4. Subcutaneous absorbable sutures (4-0 or 5-0 Vicryl or Monocryl [Ethicon]) are useful to help close the deep lacerations, but should be kept to a minimum to reduce tissue reaction in the wound. It is helpful to start in the middle of the laceration to aid in lining up the edges correctly.
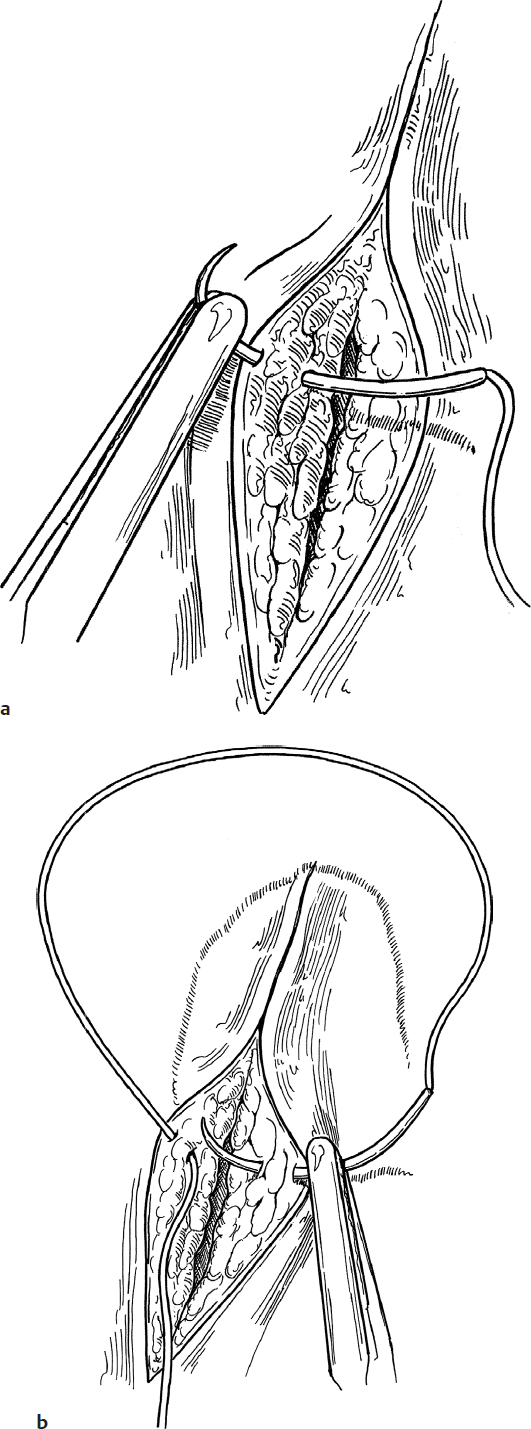
5. The skin is closed with interrupted buried subcuticular absorbable sutures when possible (Fig. 36.1a,b,c).
6. Attention is given to take a larger “bite” of the dermis and subcuticular tissue than the epidermis in order to evert the wound and bury the knot (Fig. 36.1d).
7. Wound tape or tissue adhesives are then applied to reduce skin tension (Fig. 36.1c,e).
8. If an interrupted subcutaneous closure is not possible, an interrupted closure with 5-0 or 6-0 fast-absorbing surgical gut (which usually do not need to be removed) or nylon can be used, again being careful to evert the wound edges (Fig. 36.1e,f).
9. Wound tape can be applied across the closure to reduce wound tension, if desired (Fig. 36.1e).
10. Facial sutures are removed at 3 to 4 days to prevent stitch marks. Neck sutures are removed in 4 to 6 days.
Complications
1. Widened/hypertrophic scar
2. Keloid
3. Uneven skin edges
4. Infection
5. Wound dehiscence