CHAPTER 50 Eyelid reconstruction

Anatomy
The basic structure of the eyelids is a composite of two layers, or lamellae – an anterior lamella of skin and orbicularis muscle and a posterior lamella of tarsal plate and conjunctiva. The gray line marks the junction of the lamellae at the lid margin (Figs 50.1, 50.2).
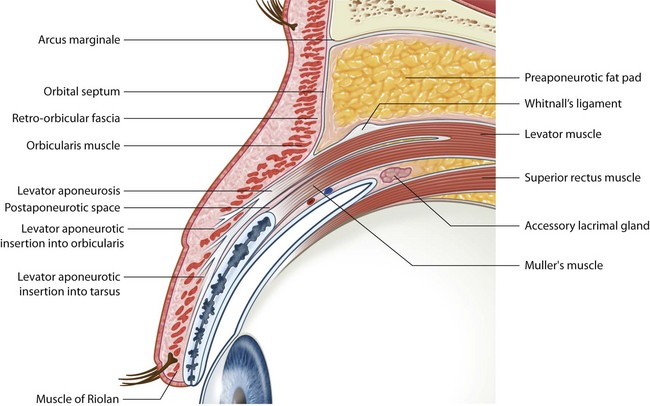
Fig. 50.1 Section through the upper eyelid.
From Tyers & Collin. Color Atlas of Ophthalmic Plastic Surgery. 2008, Elsevier, Butterworth-Heinemann.
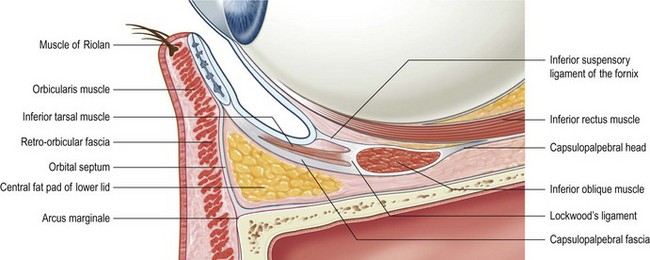
Fig. 50.2 The canthal tendons.
From Tyers & Collin. Color Atlas of Ophthalmic Plastic Surgery. 2008, Elsevier, Butterworth-Heinemann.
The lids are supported at each end by canthal tendons which are attached to the tarsal plates and the orbicularis muscle. The medial canthal tendon is a complex structure, but its essential feature, for the purposes of eyelid reconstruction, is a firm attachment to the posterior lacrimal crest. The lateral canthal tendon attaches to Whitnall’s tubercle just within the lateral orbital rim (Fig. 50.3).
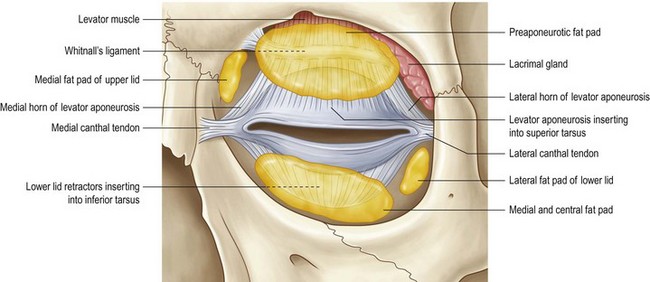
Fig. 50.3 Section through the lower eyelid.
From Tyers & Collin. Color Atlas of Ophthalmic Plastic Surgery. 2008, Elsevier, Butterworth-Heinemann.
Fundamental principles
Incisions
The ‘relaxed skin tension lines’ (Langer’s lines) mark the preferred direction of skin incisions anywhere on the body surface. In the periocular region they are generally parallel to the lid margins (Fig. 50.4).
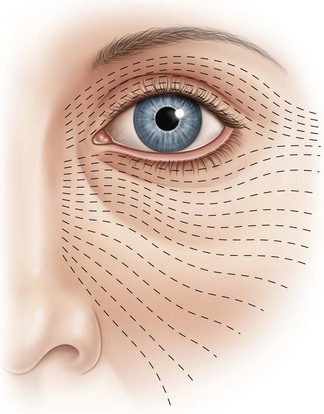
Fig. 50.4 Relaxed skin tension lines around the eye.
From Tyers & Collin. Color Atlas of Ophthalmic Plastic Surgery. 2008, Elsevier, Butterworth-Heinemann.
Correctly placed incisions result in good healing with the least scarring.
Posterior lamellar flaps
If a skin graft is to be used for reconstruction of the anterior lamella of a full-thickness eyelid reconstruction, the posterior lamella must be a flap with an intact blood supply. Few are available. The most commonly used is a tarso-conjunctival flap from the upper lid for reconstruction of lower lid defects (see Landolt–Hughes tarso-conjunctival flap below). An alternative for lower lid defects is the Hewes flap, which is an upper tarsal flap based laterally (see below).
Composite flaps
An alternative to the reconstruction of each eyelid lamella separately, is to use a composite flap of both lamellae. An upper lid defect may be reconstructed with a flap of full-thickness lower lid (see Cutler Beard procedure below). A lower lid defect cannot be reconstructed in this way with a full-thickness flap from the upper lid.



