CHAPTER 46 Eyelid malpositions
Entropion and ectropion

Introduction
Intact eyelids cover the eye completely while closed and the lid margins stay in direct contact with the globe while opened1. The lid margin’s contact line to the ocular surface is of vital importance to the integrity of the ocular surface. Dysfunction of lid motility and position can lead to symptoms varying from mild discomfort and dry eye to severe corneal ulceration and sight-threatening ocular surface disease. It is therefore most important to address lid malposition with the appropriate surgical therapy2–4. (Further suggested reading).
Entropion is a condition in which the lid margin is turned inward onto the ocular surface, while ectropion by definition is the contrary, describing a lid margin that turns outward, leading to exposure of tarsal conjunctiva (Figs 46.1 and 46.2).


Preoperative assessment
Operation techniques
Lower lid ectropion
Tarsoconjunctival excision
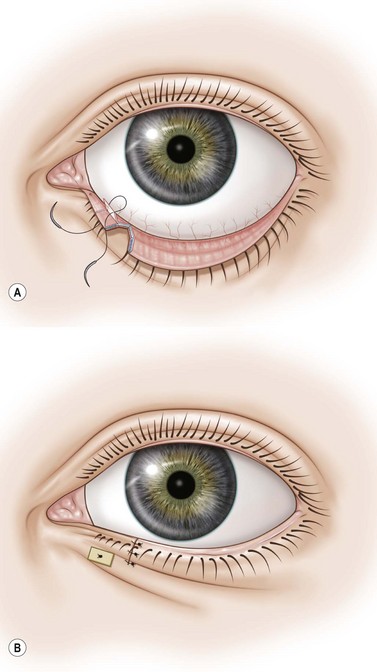
If the canthal tendon is tight and ectropion of the medial third of the lid has led to eversion of the lower punctum, an excision of the posterior lamella with or without plication of the lower lid retractors is sufficient to correct the problem5.
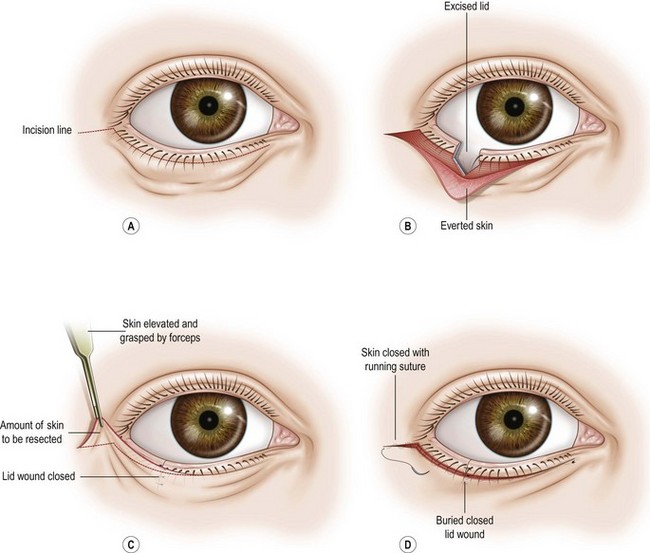
(Tarso)conjunctival excision, inverting sutures, and horizontal lid shortening (lazy T procedure)
If the canthal tendons are tight and the eversion is mainly in the medial third of the lid, inverting the lid margin by excising a part of the conjunctiva and shortening the lid horizontally will correct the malposition. The resulting incision lines after closure forms a T that lies lazily on its side, hence the name6.