Chapter 4
EYE INJURY EPIDEMIOLOGY AND PREVENTION OF OPHTHALMIC INJURIES

Epidemiology involves systematic observation (data collection) leading to the development and execution of a strategy (planning and implementing an intervention). Subsequent observation (testing the efficacy of the intervention) determines whether the recommended strategy (preventive measure) has been successful.
SPECIAL CONSIDERATION
Epidemiology was born during the fight against infectious disease, one of the two major causes of early death throughout recorded human history. Trauma, the other major cause of early death, has long been considered a result of random, unrelated, and unpreventable factors rather than a disease and, as such, has received far less attention.
Through the development of scientific and public health models, injuries are now defined and measured; and interventions are designed, tested for effectiveness, and implemented if their efficacy is proved.
PEARL… Injuries are no longer perceived as unavoidable events.
Although the eyes represent only 0.1% of the total body surface and only 0.27% of the anterior body surface, their significance to individuals and society is disproportionally higher: most of the information reaches humans through vision. Consequently, the socioeconomic impact of ocular trauma can hardly be overestimated. Those affected often have to face:
• loss of career opportunities;
• major lifestyle changes; and, occasionally,
• permanent physical disfigurement.
In addition to the physical and psychological1 costs of eye injuries to the individual, the direct and indirect financial costs to society are enormous (Table 4–1). The cost-effectiveness of well-planned preventive measures based on sound epidemiologic data has repeatedly been demonstrated.2–4
In industrialized nations, trauma has become the most common reason for extended hospitalization of ophthalmologic patients. In the United States alone5 there are almost 2.5 million incident cases of eye injuries each year; the number of people with trauma-related visual impairment was close to 1 million in 1977 with 40,000–60,000 incident cases of trauma-related visual impairment annually.
THE UNITED STATES EYE INJURY REGISTRY
The prerequisite for the scientific study of injury is acquisition of data6 to design appropriate preventive and therapeutic interventions; the same surveillance system is used to monitor the effectiveness of preventive, acute care, and rehabilitative interventions.
| Publication Year, Reference | Finding | Remark | ||
|---|---|---|---|---|
| 199042 | Hospital charges for ocular injuries: $200 million each year | Excluding those admitted to the Veterans Administration system, physicians’ fees, outpatient follow-up charges, medication expenses, and indirect costs | ||
| 19889 | Those with open globe injuries lose an average 70 days of work | This generates additional indirect costs | ||
| 19889 | 40% of those with work-related open globe injuries pursue legal action | This generates additional indirect costs | ||
| 2001* | Total cost in 1995 of the 140,000 disabling eye injuries at the workplace: $3,920,000,000; of this, the total direct cost of workers compensation claims was $924,840,000 | When the cost of nondisabling eye injuries is included, the total easily exceeds $4 billion |
* Prevent Blindness America Statement on the Scope of the Eye Injury Problem, Schamburg, IL.
PEARL… Prevention requires developing and maintaining a comprehensive and standardized eye trauma surveillance system in a defined population7 to identify risk factors.
Established in 1988,8 the USEIR satisfies the following criteria:
• collects information at hospitals and emergency rooms as well as at physicians’ offices;
• uses single-page initial and 6 months follow-up reporting forms (Figs. 4–1 and 4–2 );
• surveys all types of eye injuries—open globe, closed globe, and adnexal; but
• limits data collection to injuries resulting in permanent and significant structural or functional change to the eye.a
In the USEIR, the reporting forms as well as the data collecting and handling processes are standardized (see Chapter 1) and, regardless of whether the information is sent in paper or electronic format (floppy or zip disc or via the Internet), the data undergo multiple quality checks before becoming available for research.
Although an eye injury is a sudden and usually unanticipated event to the person involved, general trends can be identified if the surveillance is on a sufficiently large scale, such as in the USEIR. Its affiliates currently operate in 25 countries,b allowing comparison of findings from different geographic locations or across national borders and making it easier to highlight areas amenable to prevention.c
OCULAR TRAUMA EPIDEMIOLOGY: GENERAL FINDINGS
Annual Incidence Rated of Hospitalization for Eye Injuries
The annual incidence rate of hospitalization for eye injuries is 8.1 in Scotland13; 12.6 in Singapore7; 13.2 in the United States14; and 15.2 in Sweden15.
Cumulative Lifetime Prevalencee
The cumulative lifetime prevalence of eye injuries is 86016 to 14,40017; see Table 4–2 for additional information.
Who is at Risk
• Approximately 80% of those injured are males;17–22 male/female ratio in the USEIR is 4.6 : 1 and in the HEIR is 4.3 : 1.
• Most of those injured are young with an average age around 30 years.9,18,21,22 The average age in the USEIR is 33 years and in the HEIR is 29 years. Patients younger than 30 years in the USEIR: 57% and in the HEIR: 42%. The age range in the USEIR is 0–101 years and in the HEIR is 0–85 years. The estimated risk of sustaining ocular trauma when two persons are compared is 80% higher for the individual who is 10 years younger.19
• Less educated and less wealthy persons are more prone to partake in risk-taking activities and thus to be injured.18,19
• Nonwhites have a 40 to 60% higher risk.22 Black or Hispanic races in the United States are more at risk between ages 25 through 65 years.
• The combined effect of race and sex cannot be ignored: in one survey, 23% of black men, 20% of white men, 12% of black women, and 8% of white women reported at least one injury in their lifetime.17
• Other risk factors include self-reported dangerous behaviors (e.g., traffic violations, marijuana use)19; and alcohol and drug use, unemployment, and unsettled social environments12.
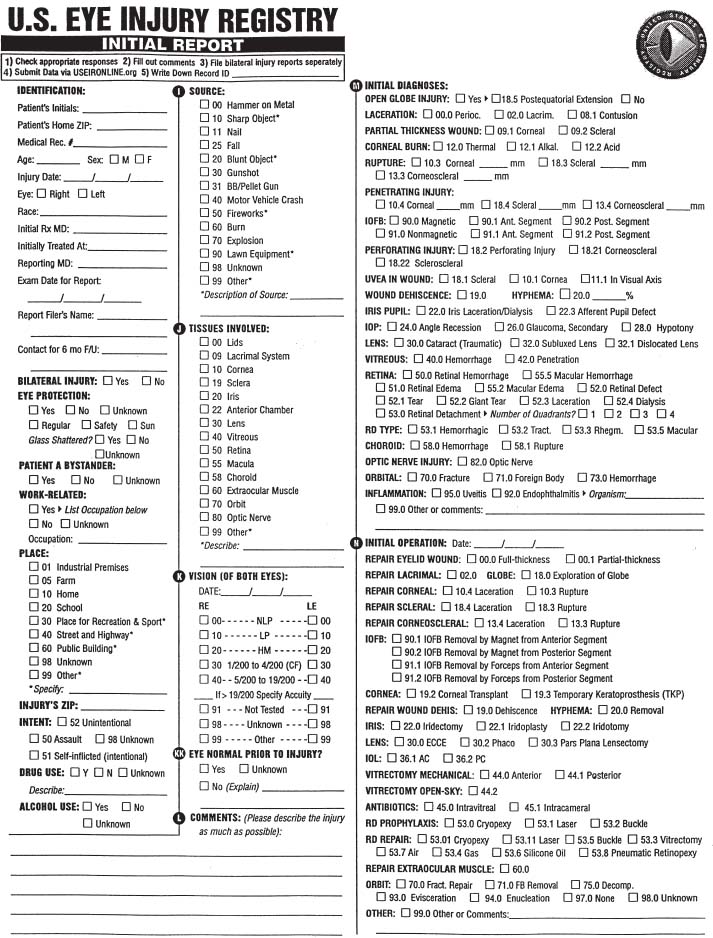
FIGURE 4–1 The revised initial reporting form of the USEIR.
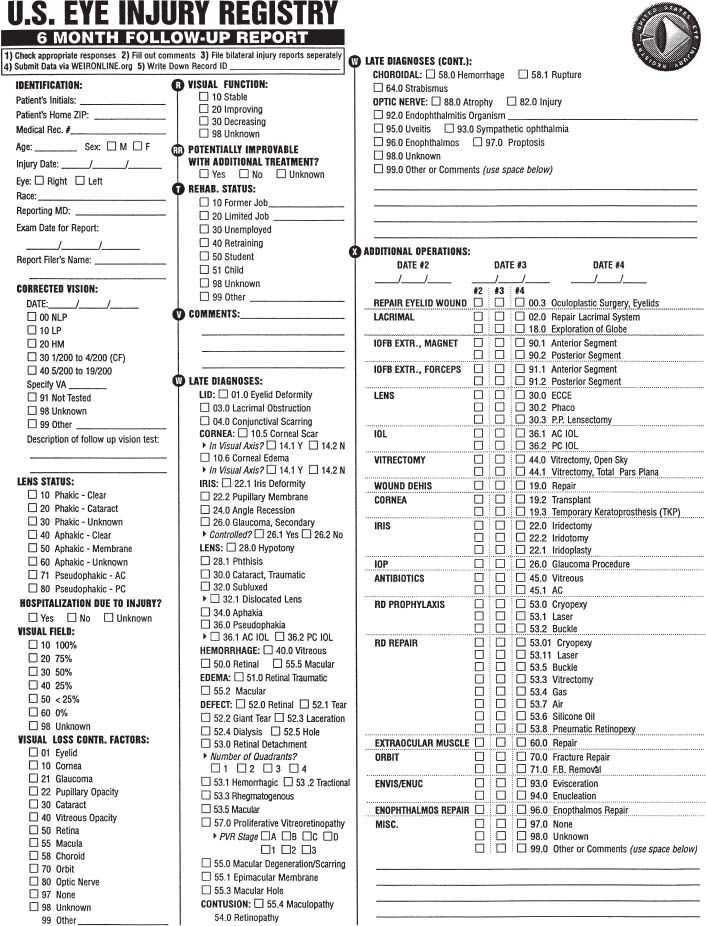
FIGURE 4–2 The revised 6-month follow-up reporting form of the USEIR.



