Chapter 16
EXTRABULBAR TISSUE PROLAPSE

The primary objective in managing injured eyes is to reestablish the original anatomy and function.1,2 Proper handling of prolapsed tissues is essential to achieving a good outcome.3 In this chapter we provide guidelines regarding the indications and techniques of treating tissue prolapse, a common finding in open globe trauma. The incidence of tissue prolapse is:
• 42% (USEIR) to 45% (México City, 1991a) in open globe injuries; and
• significantly higher in ruptures (70%) than in lacerations (49%; USEIR).
DEFINITION AND HISTORY
Tissue prolapse is defined as extrusion of intraocular content outside its normal compartment, whether intrabulbar (e.g., vitreous in the AC) or extrabulbar (e.g., expulsed lens).
Before the early 20th century, iris prolapseb through a corneal wound was considered a severe complication because of:
• fear of infection;
• fear of SO; and
• technical difficulties in management.
When topical eserine and bright light were not sufficient to return the iris to the AC, the wound was simply covered by a conjunctival flap with a purse-string suture and left to heal. Scleral wounds were treated similarly, with no intent of closure by sutures. Leeches were recommended to deal with the “congested uvea” associated with trauma.4 It was accepted that wounds involving the retina or choroid would be followed by retinal detachment and phthisis.4 Enucleation was routinely performed in cases of prolapsed ciliary body, choroid, retina, or vitreous.5,6 The vitreous was thought to hold the retina in place; consequently, its removal was prohibited.5 Even when wounds finally began to be sutured, corneal scarring and retinal detachment commonly resulted in poor visual results, which started improving only after the 1950s, with the advent of microsurgery, antibiotics, and steroids. The functional outcomes still leave room for improvement.5,7–9
PATHOPHYSIOLOGY
Tissue extruded in the context of open globe injury is usually perceived as:
• a condition complicating the initial repair; and
• a risk factor for a less favorable anatomical/visual outcome.
With the formation of a full-thickness wound, the globe’s sudden decompression may force the iris/ choroid/vitreous/retina into the wound. Because of their inside-out mechanism (see Chapter 1), ruptures have a worse prognosis than lacerations: due to the increased IOP,10–12 tissue loss is not only more common but also more severe.8,13 Other acute and chronic aggravating factors include:
• orbital and intraocular bleeding/inflammation/ injection;
• choroidal edema;
• lens swelling; and
• excessive manipulations during evaluation (Fig. 16–1).
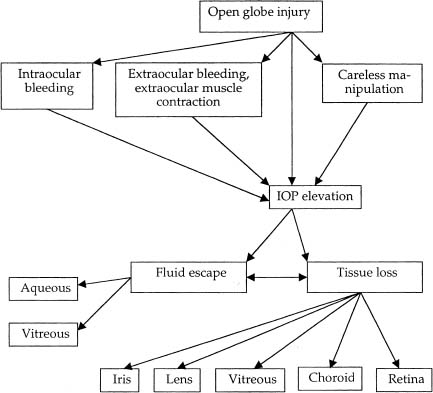
FIGURE 16–1 The pathomechanism of acute tissue prolapse.
PEARL… Tissue incarceration eventually plugs the wound, reestablishes the IOP, and tamponades the bleeding, helping to preserve the eye’s anatomy.11
The trapped prolapsed tissue is subsequently secured by fibrin formation within a few hours and fibrosis within a few days1,14 (Fig. 16–2). This may lead to:
• inadequate wound healing;
• leakage of aqueous;
hypotension;
endophthalmitis;
epithelial ingrowth;
chronic inflammation;
corneal decompensation;
dense, vascularized corneal scars;
synechia formation;
retinal detachment.
EVALUATION
PEARL… Intraocular tissue prolapse should be suspected in all open globe injuries. Remember that the wound may remain hidden (e.g., occult rupture).
Unless the wound is posterior and underneath a congested, edematous conjunctiva or blood-stained Tenon’s capsule (see Chapters 13 and 15), the tissue prolapse is usually visible upon careful inspection. The clinician should look for the following signs:
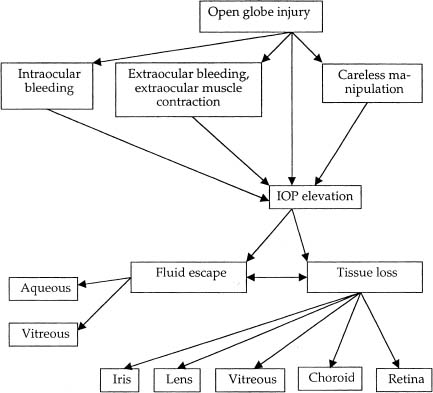
FIGURE 16–2 Photomicrograph. Uveal tissue incarcerated in scleral wound prevents adequate wound apposition and healing. (Courtesy of Dr. Alfredo Gomez-Leal, Asocoación para Evitar la Ceguera en México.)
• full-thickness eyewall defect;
• subconjunctival melanic pigment or blood;
• chemosis;
• peaked or irregular pupil;
• APD;
• hyphema;
• vitreous traction strands (best seen in the retrolental space at the slit lamp);
• vitreous hemorrhage; and
• low IOP.
PITFALL
Tissue prolapse may occur during transportation or be due to poor patient instruction and restriction and/or lack of eye shielding. As soon as an open globe injury is suspected, further diagnostic manipulations should be kept to a minimum (see Chapter 8).
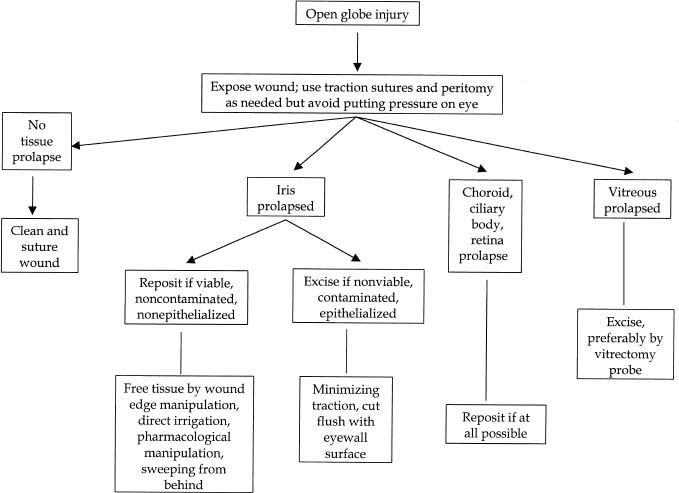
FIGURE 16–3 General management principles.
PEARL… The nonophthalmologist should shield the eye and consult an ophthalmologist regarding transportation, systemic antibiotics, and pain medication.
Preoperative echography and CT scan may show tissue prolapse in case of a posterior scleral break. Although these techniques are seldom necessary when deciding whether to explore the globe, they may aid in planning the surgery.16,17
MANAGEMENT
Heavy topical and systemic corticosteroid therapy is essential to minimize inflammation (see Chapter 8). The rules of culturing and antibiotic therapy10,18 follow the general principles for open globe trauma (see Chapter 28 and the Appendix). The implications, instrumentation, and technique of management vary with each tissue (see below and Fig. 16–3). All tissue prolapses should be addressed at the time of wound repair (Fig. 16–4).

FIGURE 16–4 Iris prolapse through limbal wound.
PITFALL
Leaving tissue prolapsed may lead to severe complications such as SO and is acceptable only if severe bleeding occurs (ECH/SCH; see Chapter 22).
Irisc (see also Chapter 18)
Conventional wisdom dictated that iris exposed for more than 24 hours should be excised for fear of introducing infected material or epithelial cells into the eye.2,10,19 With improved surgical techniques, technology, and pharmaceuticals, the surgeon should not be dogmatic about this 24-hour deadline.15
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


