Fig. 17.1
Light microscopic appearance of exfoliation material deposition on the lens surface (Courtesy of Ursula Schloetzer-Schrehardt)
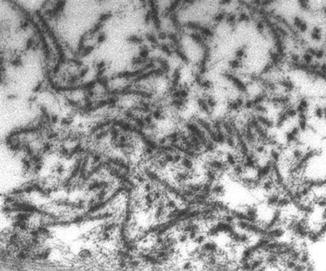
Fig. 17.2
Electron microscopic appearance of exfoliation material aggregates (Courtesy of Ursula Schloetzer-Schrehardt)

Fig. 17.3
Classic slit-lamp appearance of exfoliation material deposition on the lens. The central disc and peripheral granular zone are evident together with marked pupillary ruff atrophy
Intraocular synthesis and accumulation of exfoliation material predominantly involve the anterior segment of the eye; exfoliation aggregates are synthesized by the nonpigmented ciliary epithelial cells, trabecular endothelial cells, vascular endothelial cells in the iris, and pre-equatorial lens epithelium cells. After reaching the extracellular space, exfoliation aggregates are deposited around the cells of origin, but may also be passively transported by the aqueous humor and be deposited upon the zonular apparatus, anterior lens surface, pupillary margin, and within the outflow system. In the trabecular meshwork (together with the pigment granules liberated from the pupillary margin and the posterior layer of the iris), the accumulated exfoliation material can reduce aqueous humor outflow leading to a gradual increase of intraocular pressure (IOP) and subsequent development of XFG with optic nerve head damage. Exfoliation aggregates have been identified in many different systemic organs, such as connective tissues, skin, heart muscle cells, striated muscle cells, and large vessel walls [10].
Exfoliation material is not only synthesized and accumulated in different tissues, but more importantly by disturbing extracellular matrix metabolism, it can induce alterations in function [1, 2, 12]. These XFS-related degenerative changes are clinically important and must be known by all ophthalmologists (Fig. 17.4). First, XFS causes zonular fragility and disruption that subsequently may lead to lens subluxation, which results in surgical complications during phacoemulsification cataract surgery and in extreme cases may lead to pupillary block or secondary angle-closure glaucoma. The zonular fragility, thinning of the equatorial lens capsule, and reduced dilatation of the pupil are thought to be responsible for the increased complication rate during cataract surgery, as well as the postoperative decentration of intraocular lenses even years after uncomplicated cataract surgery. In some cases, exfoliation-induced corneal degenerative changes may impact the number and shape of corneal endothelial cells, which may lead to corneal decompensation even after uncomplicated phacoemulsification cataract surgery or following marked elevation of IOP [3].
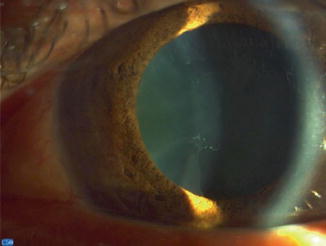
Fig. 17.4
Biomicroscopic appearance of an eye with exfoliation syndrome. A subtle bridge connects the central disc with the peripheral granular zone
The degenerative changes induced by XFS and XFG in the iris result in the reduced pupillary dilatation in these patients. Further, degenerative changes and exfoliation deposits around the wall of iris vessels lead to micro-occlusions, formation of ghost vessels (Fig. 17.5), and secondary micro-neovascularization. These changes are important clinically since they result in increased vascular permeability and impairment of the blood-aqueous barrier function, which can lead to increased incidence of posterior synechiae formation and more severe inflammation after intraocular surgery. Retrobulbar perfusion may also be impaired in XFS and XFG.
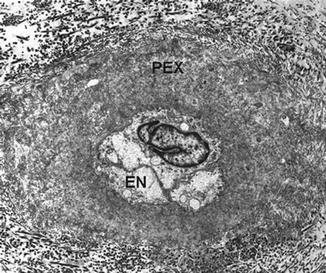
Fig. 17.5
Ultrastructural appearance of an iris ghost vessel. Exfoliation material (PEX) completely surrounds the obliterated lumen of the vessel. EN endothelium of the vessel (Courtesy of Ursula Schloetzer-Schrehardt)
Systemic Diseases in XFS
Though rarely appreciated by ophthalmologists, XFS patients may also exhibit systemic vascular involvement. There are now several reports of impaired regulation of heart function and reduced precapillary perfusion [12, 13]. In the large vessels, rigidity increases and elasticity decreases compared to the age-matched elderly population [14]. Plasma homocysteine level is also increased in XFS and XFG, and homocysteine level increases with the duration of XFS [14]. Since disturbed homocysteine metabolism and the consequent increase of the plasma homocysteine level are responsible for several serious vascular diseases including ocular vascular occlusions (e.g., retinal vein occlusion [15–18]), XFS/XFG patients with a positive vascular history can benefit from a consultation with an internist or a cardiologist. These systemic alterations can explain why XFS is frequently associated with systemic vascular diseases [13]. At present, however, we do not recommend performing homocysteine level testing routinely in these patients. Though the vascular diseases are considered a consequence of disturbed extracellular material metabolism in XFS, no connection was found between the frequencies of the risk alleles of LOXL1 polymorphisms and the presence of systemic vascular diseases [17].
XFS and XFG are systemic disorders with several ocular and extraocular sequelae.
Evolution of XFG from XFS
Both XFS and XFG may present clinically as unilateral disease. In clinically apparent unilateral disease, ultrastructural investigation of the clinically unaffected fellow eye can often document the morphological presence of exfoliation material.
In 10 years, one-third of the clinically unilateral exfoliation cases convert to bilateral disease, whereas 30 % of the XFS eyes without IOP elevation convert to XFG.
Thus, unilateral XFS may only be a cross-sectional clinical category and not a true biological entity. This issue is of practical importance, since clinically detectable XFS or XFG often develops in the fellow eye over time [19, 20]. Statistically, over a period of 10 years, approximately one in three cases of clinically unilateral exfoliation cases convert to bilateral exfoliation [20]. The implication is that careful slit-lamp examination is required at each follow-up visit, and reconsideration of the classification of the fellow eye may be necessary if exfoliation material or elevated pressure occur.
The cumulative risk for XFG development in eyes with manifest XFS but without IOP elevation is approximately 30 % in 10 years, and most of these cases convert within the first 5 years [19]. Pressure elevation is an important indicator of the conversion process. It is thought that IOP elevation in XFS and XFG is caused by blockage within the trabecular meshwork by exfoliation material and pigment granules released from the posterior iris layer and pupillary margin. It seems likely that the meshwork becomes overwhelmed with a loss of functional reserve for handling the exfoliation and pigment deposits, and it may be that the macrophage response of trabecular cells is no longer able to deal with the abnormal material. Subsequent development of IOP elevation and exaggerated 24-h IOP fluctuation lead to optic nerve head damage, and from this point the condition is classified as XFG. The presence of exfoliation in ocular hypertension doubles the risk of glaucoma development.
Clinical Diagnosis of XFG
The clinical diagnosis of XFG relies upon the clinical detection of exfoliation material [1]. In the fully developed form of XFS, exfoliation material is visible on the anterior lens surface in a typical configuration. The relatively homogenous central disc corresponds to the size of the undilated pupil. The central disc is surrounded by a clear intermediate zone. The peripheral zone is a granular, often layered ring of exfoliation material deposits. This classic presentation, however, is not always evident, and there are subtle signs of the condition years before the classic appearance. It is important to recognize that even when it is typically present, it is common that XFS cannot be visualized without pupil dilatation. In the early stage of the disease when the classic pattern is often not yet fully developed, exfoliation material may only be seen on the peripheral part of the anterior lens capsule. Detection of the early exfoliation signs can be facilitated using low intensity slit-lamp illumination. The beam should be positioned at approximately 45° from the axis of observation. Fine exfoliation aggregates can often be visible upon the pupillary margin and less frequently on the iris, corneal endothelium, and sometimes may be seen with gonioscopy upon the trabecular meshwork. Due to the degenerative changes associated with the condition, the iris is atrophic, with transillumination defects, and the pupillary margin can demonstrate a moth-eaten appearance due to loss of pigment. Nuclear cataract is more common in XFS and XFG. In some cases, phacodonesis, subluxation, or even luxation of the lens can occur as consequence of zonular damage. Iris pigment liberation and deposition are early and typical signs in the condition. Pigment granules are frequently seen deposited on the anterior lens surface after pupil dilatation. Fine pigment deposits are commonly seen on the iris surface and less frequently upon the corneal endothelium. Pigment accumulation in the angle is pathognomonic of the condition and is seen as a wavy pigment deposition above Schwalbe’s line (called Sampaolesi’s line) and as dense, dark pigment accumulated unevenly within the trabecular meshwork (Fig. 17.6). The amount of pigment granules varies considerably and correlates well with the severity of the disease.
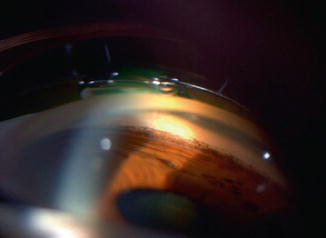
Fig. 17.6
Typical gonioscopic appearance of an eye with exfoliative glaucoma (XFG). Dense, uneven pigmentation can be seen below Sampaolesi’s line
In XFG, all characteristics of XFS are present (Fig. 17.7), accompanied by elevated IOP and an optic nerve head showing typical glaucomatous neuroretinal rim loss [21–23]. This is usually diffuse and in many cases very advanced when the diagnosis is made. The diffuse optic nerve head damage is due to the high pressure characteristics of XFG where IOP can in some instances be as high as 60 mmHg at diagnosis [22]. XFG is characterized by worse 24-h characteristics than primary open-angle glaucoma (POAG) [21]. Despite the high pressure characteristics, XFG is usually asymptomatic and not associated with pain or discomfort. Due to its unilateral presentation or the different degree of severity between the two eyes, the patient’s realization of visual loss can be delayed. Owing to the large 24-h IOP fluctuation in XFG, IOP assessment should not rely on a single pressure reading; ideally a 24-h IOP curve should be carried out or at least a daytime pressure curve with three IOP readings (morning, afternoon, and evening).
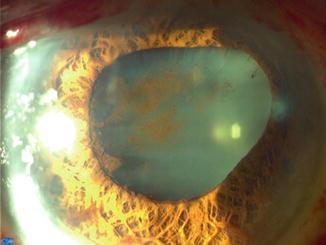
Fig. 17.7
Dense deposition of pigment on the surface of the lens together with posterior synechiae following intense dilatation of the pupil in an eye with XFG
It is necessary to establish the correct diagnosis and identify the IOP peaks in XFG management. An IOP curve is also valuable in evaluating the true magnitude of IOP reduction in XFG. Practitioners are often reluctant to perform diurnal curve studies as part of their routine evaluation of their glaucoma patients, but it is important to realize that in XFG, proper diagnosis and management cannot be obtained on the basis of a single IOP measurement.
When the pupil is pharmacologically dilated in XFS and XFG (which is vital to establish the diagnosis), pigment is frequently released from the posterior iris layer. This may result in acute pressure elevation. In order to prevent acute damage due to this IOP spike, the pressure should ideally be measured 2–3 h after dilatation and if necessary, additional IOP lowering medication should be employed.
XFG is characterized by worse 24-h IOP characteristics than POAG. A single IOP measurement is often insufficient to evaluate the real IOP in this glaucoma. A pressure curve may better delineate pressure characteristics and facilitate diagnosis and management.
Differential Diagnosis of XFG
In order to provide tailor-made management, XFG must be differentiated from other glaucoma types [1, 23]. In POAG, there is no clinical evidence of exfoliation material and the IOP characteristics (e.g., IOP fluctuation) are better, the disease is typically bilateral, there are no pigmentary signs, and optic nerve head damage is generally less severe. Though IOP in juvenile open-angle glaucoma is usually high, the patients are much younger that XFG patients. Young age is also a key differential with pigmentary glaucoma where pigmentary signs and IOP characteristics resemble those of XFG. Further, in pigmentary glaucoma, the extent of pigment liberation is greater, iris transillumination defects are typically radial, pigment deposits upon the cornea endothelium form a central vertical spindle (Krukenberg’s spindle), and the trabecular pigmentation is dense and homogeneous.
Occasionally, exfoliation and pigment deposits on the corneal endothelium are incorrectly ascribed inflammatory precipitates. Thus, XFG should also be differentiated from uveitic glaucoma. Since narrow angle, high IOP, and anterior movement of the lens due to zonular weakness can be seen in XFG just like in angle-closure glaucoma, these two glaucomas are sometimes difficult to differentiate. They often can be distinguished by their different natural course and history and via indentation gonioscopy. Finally, exfoliation keratopathy should be distinguished from Fuchs’s dystrophy (which starts in the center and spreads to the periphery later) as well as pseudophakic or aphakic bullous keratopathy (which starts on the periphery and progresses to the central cornea).
XFG should be differentiated from POAG, juvenile open-angle glaucoma, pigmentary glaucoma, uveitic glaucoma, and primary angle-closure glaucoma.
Medical Therapy for XFG
Exfoliative glaucoma is a leading cause of visual loss in the elderly and can carry a poor prognosis in some instances. It is thought to be a more severe glaucoma with faster progression than POAG [1, 2, 24]. This is due to several clinical characteristics including older age, higher mean and peak IOP, wider 24-h IOP fluctuation, and more visual field damage at diagnosis. It has never been elucidated to date whether the worse prognosis in XFG is due to the difference in age, the worse 24-h IOP characteristics of XFG, or to a poorer response of XFG to medical therapy [25–27]. Although published literature suggests that XFG generally responds less well to medical therapy than POAG, this may simply reflect the worse IOP characteristics in XFG [28]. Previous studies suggest that absolute IOP reduction and the percentage fall of pressure with medical therapy in XFG are often higher than in POAG. Nevertheless, in many XFG cases, it is more difficult to reach the predetermined target IOP with monotherapy [29]. Therefore in XFG, more medication becomes necessary to control the pressure and laser or surgical intervention are more often required.
In patients with XFG, there is a dose–response relationship between levels of IOP lowering and the subsequent rate of progression [25]. There is a strong linear correlation between untreated 24-h IOP characteristics and mean visual field defect at diagnosis [21]. In the first study that evaluated target pressure in XFG and the influence of IOP reduction on the long-term stability or progression within 5 years, XFG patients with a mean IOP ≤ 17 mmHg progressed only 28 % of the time compared with 70 % of XFG cases that progressed with a mean IOP ≥ 20 mmHg [26]. Stepwise, medical therapy in XFG is currently similar to POAG. It is likely, however, that future medical therapy in XFG will be different from that employed in POAG. Medical therapy includes beta-adrenergic antagonists, alpha-adrenergic agonists, miotics, carbonic anhydrase inhibitors, and prostaglandin analogues. Despite the arrival of new classes of topical medications, which have significantly reduced the rate of surgery in XFG (just like in POAG), the trend remains for XFG to respond less well to monotherapy, to require more often adjunctive therapy, maximal medical therapy, and, finally, to require sooner and more often surgical intervention. At the present time, the impact of new medications on the long-term prognosis of XFG remains unknown [27].
In XFG, response to timolol has been reported to be less favorable than in POAG [25, 28, 30, 31]. In a 24-h study, despite a greater mean 24-h IOP reduction with timolol, XFG patients still exhibited worse 24-h IOP characteristics and greater fluctuation of IOP than age-matched patients with POAG [30]. However, the short-term as well as the long-term success rates of IOP control with timolol therapy are low. Indeed, only 8 % of XFG patients versus 33 % of POAG patients were successfully controlled with timolol monotherapy after 3 years [30]. Dorzolamide was documented to be efficacious as monotherapy in XFG [32]. In another study [33], dorzolamide was additive to timolol over 24-h but it did not alter the worse IOP characteristics compared with POAG.
In a parallel study in 50 XFG patients, the fixed combination of dorzolamide/timolol was found to provide significantly greater diurnal IOP reduction (45 %) compared with either latanoprost (34 %) or travoprost (36 %) monotherapy [34]. This means diurnal reduction was greater than that reported for POAG patients with these drugs. The dorzolamide/timolol fixed combination has also been evaluated as initial therapy in XFG and was found to be a viable option [35]. In a crossover study, Konstas and associates [35] employed this fixed combination as initial therapy in 65 newly diagnosed patients with XFG with a mean pretreatment IOP of 31.2 mmHg. After 2 months of therapy, the fixed combination provided a mean reduction of 13.1 mmHg (42 %) at peak.
To date there is limited information for the response and success rate with the prostaglandin analogues in XFG. In a recent prospective parallel diurnal study, latanoprost was slightly more effective than timolol monotherapy in lowering IOP in eyes with XFG [36]. There was a trend for better diurnal IOP control and significantly less diurnal IOP fluctuation with latanoprost therapy.
In a parallel study [34], travoprost was found to obtain similar reduction in diurnal IOP (36 %) in patients with XFG compared with latanoprost (34 %). In a more recent crossover study, however [37], in 42 XFG patients, mean 24-h IOP with travoprost (17.3 mmHg) was significantly better than that with latanoprost (17.8 mmHg), and this difference was attributed to significantly better IOP control with travoprost at 18:00 (16.7 mmHg versus 17.9 mmHg). A recently published study investigated the efficacy of bimatoprost compared with latanoprost in XFG [38]. This multicenter, crossover, 3-month study investigated the diurnal IOP control obtained with bimatoprost versus latanoprost in 129 consecutive XFG patients. Bimatoprost obtained significantly lower diurnal IOP than latanoprost (17.6 mmHg versus 18.6 mmHg) after 3 months of chronic therapy. In a recent meta-analysis of 24-h studies, the results of prostaglandin monotherapy for patients with XFG demonstrated in general that both untreated baseline and treatment arms were higher in XFG and the 24-h IOP reductions from baseline were greater than observed in the POAG patients [39].
Adjunctive latanoprost therapy is safe and well tolerated for the long-term treatment of patients with XFG [27, 40]. One study reported that latanoprost is more effective as adjunctive therapy with timolol than dorzolamide [40]. The role of fixed combinations (e.g., dorzolamide/timolol, latanoprost/timolol, travoprost/timolol, bimatoprost/timolol, and brimonidine/timolol fixed combinations) in the medical therapy of XFG requires further elucidation. In certain XFG patients with high baseline IOP and advanced damage, fixed combinations may be the best initial choice for therapy. It is conceivable that these XFG patients will benefit from initial medical therapy with fixed combinations. In medicine, initial therapy with fixed combinations was found to provide improved clinical outcome in real life practice. Fixed combinations obtain better IOP control than concomitant unfixed therapies and reduce the incidence of adverse events. In XFG, fixed combinations should be used earlier and more frequently in the stepwise therapy of XFG because of the worse 24-h IOP characteristics, the faster progression, and worse prognosis.
Future research on the efficacy of new medications specifically in XFG may determine the best initial and stepwise therapy in this secondary glaucoma. The target 24-h IOP that will ensure stability in all XFG patients remains to be determined. Such information is especially important because XFG is a severe form of open-angle glaucoma, more often associated with vision loss than POAG. The future focus on therapy in XFG should not only be IOP reduction and will probably include innovative approaches that may slow the progression from XFS to XFG or even prevent the development of XFG.
Medical therapy is more difficult in XFG. Although the IOP reduction may be initially greater, the worse 24-h IOP characteristics in this condition make it more difficult to obtain the desired target pressure. Therefore, adjunctive therapy is often needed. Fixed combination drugs should be used earlier in XFG.
Argon Laser Trabeculoplasty in XFG
Argon laser trabeculoplasty (ALT) is a successful and well-established photocoagulative procedure for lowering IOP in XFG [41]. Most studies show a better response to ALT in XFG than in POAG; nevertheless, late failure may be more common in XFG [41–45]. Traditionally, ALT has been recommended when IOP is not satisfactorily controlled with maximum tolerated medical therapy, as an option before filtering surgery. However, when medical treatment is contraindicated and in elderly or noncompliant patients, ALT may also be a valuable option as first choice of treatment [42, 46]. XFG is characterized by dense trabecular pigmentation; therefore, XFG eyes with open anterior chamber angles are particularly suitable for ALT. Since the amount of pigmentation of the meshwork directly influences the outcome and in XFG the meshwork is generally more heavily pigmented, the power selected should be less than that selected with POAG. The optimal power setting is determined by the heat-induced reaction of the trabecular meshwork, which determines if the power setting is appropriate. Ideally, the IOP should be checked during the first 6 h postoperatively. If it is not possible, pretreatment with topical apraclonidine and the use of oral acetazolamide postoperatively is recommended to prevent an ALT-induced IOP spike. Topical steroids or topical nonsteroidal anti-inflammatory drops are to be used four times daily for 7 days. Close monitoring is suggested in cases of advanced glaucoma, one-eye patient, high pre-laser IOP, and repeated trabeculoplasty. The result of ALT cannot be evaluated before 4–6 weeks. ALT has very few complications – the commonest is a transient elevation of IOP, which is more common in XFG than in POAG. In some eyes, there is a formation of small peripheral anterior synechiae (especially after posteriorly placed burns or in patients with narrow angles). Late gradual IOP elevation due to loss of ALT effect is common. Although conceivably ALT may decrease the success of subsequent filtration surgery, there is no controlled evidence to support this hypothesis.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


