Excision of Cancer of the Buccal Mucosa
Anil K. D’Cruz
INTRODUCTION
Cancers of the buccal mucosa are a global problem. The incidence varies from 40% to 60% of all cancers of the head and neck in South Asia to about 10% in North America and Western Europe. The main reason for this disparity is the use of smokeless tobacco in South Asia. Quid (paan), which is a combination of areca nut, slaked lime, and tobacco, is usually kept in the gingivobuccal sulcus for prolonged periods of time exposing the mucosa to multiple carcinogens.
Cancer of the buccal mucosa usually presents late and behaves more aggressively when compared to carcinomas of other subsites of the oral cavity due to the limited anatomic barriers within the buccal space. A high rate of locoregional recurrence (26% to 80%) after treatment is the most common cause of mortality in this group of patients. Surgery is the mainstay of treatment for these cancers and therefore needs to be planned accurately and executed appropriately to give the patient the best chance for cure.
HISTORY
Cancer of the buccal mucosa is associated with few symptoms in the early stages, and an accurate history is imperative to establish an early diagnosis. The most common presentation is a patch or a nonhealing ulcer in the oral cavity. Any such lesion, particularly in a tobacco/alcohol user, that persists more than 6 weeks warrants speciality consultation and investigation. In those without a history of addiction, a history of carious and sharp teeth should be sought. History of pain usually signifies deep infiltration of a locally advanced cancer. Recent onset of trismus is indicative of involvement of the infratemporal fossa, a sign of relative inoperability. This must be differentiated from a history of long-standing trismus, which may be associated with submucous fibrosis, a peculiar premalignant condition seen in patients in Southeast Asia who consume Areca nut (Fig. 3.1). Loosening of teeth is indicative of invasion of the adjacent alveolus. Patients who have advanced cancer may present with fullness in the region of the hemiface and erythema or ulceration of the skin.
PHYSICAL EXAMINATION
Lesions must be carefully examined to help in accurate surgical planning. The location of the cancer in relation to the commissure anteriorly, retromolar trigone posteriorly, upper alveolus superiorly, and lower alveolus inferiorly must be assessed both visually and by digital palpation. Very often, contiguous bone involvement can be suspected clinically even before imaging. The skin overlying the ulcer must be examined for puckering, tethering, or frank invasion. Cancer of the buccal mucosa may be associated with a coexisting premalignant condition, and the entire oral cavity must be carefully inspected.
 FIGURE 3.1 Oral submucous fibrosis with trismus. |
Occasionally in patients who have severe pain and trismus, examination may need to be performed under a brief general anesthesia. Inadequate mouth opening (pseudotrismus due to pain and masseter spasm) may be relieved after the administration of general anesthesia. This facilitates proper evaluation of the extent of the lesion in the oral cavity.
Cancer of the buccal mucosa has a lower propensity to metastasize to the cervical lymph nodes when compared to cancer of the tongue. The first echelon of nodal spread is usually Level I (submental and submandibular). The entire neck must be carefully examined for metastatic lymph adenopathy.
Two additional areas of particular importance that must always be examined are soft tissue involvement by tumor in the paramandibular region and its relationship to the zygoma superiorly. For paramandibular spread of the tumor, involved soft tissues are checked for mobility with relationship to the mandible by palpating the cheek from the exterior (Fig. 3.2). In those cancers that do not move freely on the mandible, a marginal mandibulectomy may not be feasible even if bone is not radiologically eroded on imaging. If induration extends superiorly to the zygoma, achieving negative margins is difficult and the patient should be considered inoperable. It is a good clinical practice to use bimanual palpation to assess the superior extent of the cancer.
Careful examination of the dentition is critical to look for dental caries, periodontal disease, and fractured sharp teeth. Hypoesthesia in the region of the chin is suggestive of involvement of the inferior alveolar nerve.
Lastly, as in all cancers of the head and neck, a thorough endoscopic examination of the entire upper aerodigestive tract is warranted to look for synchronous second primary cancers.
INDICATIONS
Surgery is the mainstay of treatment for cancer of the buccal mucosa, and all operable lesions should be considered for excision if the patient is fit for general anesthesia. The indications for surgery would therefore be all lesions clinically staged T1 to T4a.
 FIGURE 3.2 Mobility of soft tissue over the mandible is checked in the presence of paramandibular spread to assess for feasibility of marginal mandibulectomy. |
The extent and approach for excision would vary depending on the clinical T stage. Lesions should therefore be assessed for suitability of approach (per oral or via cheek flap) and for the need of excision of adjoining mandible (marginal or segmental mandibulectomy).
Early superficial accessible midbuccal lesions are approached perorally. A cheek flap approach is necessary in patients with restricted mouth opening (trismus), lesions located posteriorly, in larger tumors and those requiring mandibulectomy.
If the lesion abuts or is superficially eroding the mandible, a marginal mandibulectomy is advisable. Advanced lesions with gross invasion of the mandible or lesions with significant paramandibular spread require segmental mandibulectomy for oncologic adequacy. The specific indications and contraindications to various surgical approaches are discussed in respective sections.
CONTRAINDICATIONS
Contraindications to surgery can be divided broadly into two groups: those associated with fitness for surgery and those with advanced cancer factors. Cardiovascular disease, pulmonary disease, compromised renal function, and uncontrolled diabetes that render the patient unfit for general anesthesia preclude surgery. Locally advanced cancers staged T4b are contraindications to surgery, namely, involvement of the masticator space (Fig. 3.3), destruction of the pterygoid plate, involvement of the skull base, and cancer encasing the internal carotid artery. Extensive involvement of skin and soft tissue is also a contraindication to surgery. These include induration extending to the zygoma, diffuse edema of the hemiface, and multiple skin nodules.
Involvement of the infratemporal fossa was traditionally considered a sign of inoperability. However, recent evidence suggests that involvement of the infratemporal fossa into the notch (cancer inferior to the sigmoid notch) may be amenable to surgery with reasonable possibility of control. In a study conducted by Liao et al., the disease-free survival in infranotch and supranotch T4b cancers of the oral cavity was 64.7% and 14.3%, respectively, with overall survival of 55.3% and 14.3%, respectively (Figs. 3.4 and 3.5).
PREOPERATIVE PLANNING
Imaging
Imaging should be performed in all cases of cancer of the buccal mucosa as it provides valuable information with regard to extent of the cancer. The only exception would be in very early superficial cancers with a clinically node-negative neck where peroral excision is planned. Ultrasound examination of the neck is all that needs to be done to identify subclinical nodal metastasis if observation of the neck is contemplated.
 FIGURE 3.3 Coronal 16-slice contrast enhanced computed tomography (CECT) reformation defining the boundary of the masticator space (enclosed by the white line that represents slips of the investing layer of cervical fascia). (m, masseter muscle; asterisk, lateral pterygoid muscle; short arrow, medial pterygoid muscle.) |
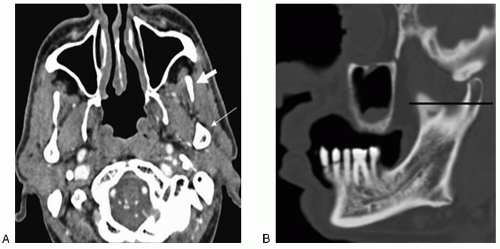 FIGURE 3.4 A: Axial CECT at the level of the mandibular notch; thick arrow shows coronoid process; thin arrow shows condyle. B: Modified oblique reformation on 16-slice CT (bone window) shows black line demarcating supra- and infranotch levels (high and low infratemporal fossa). |
CT and MRI scans both have their advantages and are complementary to each other. CT scan is usually preferred as the initial imaging modality as it is easily available, less expensive, and preferred by most surgeons for interpretation. It gives a fair idea about the extent of the lesion, involvement of the cortical bone, and extension into the infratemporal fossa. MRI is better for the evaluation of recurrent cancer and involvement of medullary bone. Accurate assessment of the depth of infiltration and early involvement of the periosteum are sometimes hindered due to the apposition of mucosal surfaces of the buccal cavity. The puffed cheek technique described by Weissman and Carrau is a useful maneuver in such situations. In this technique the patient blows uniformly through the pursed lips, which opens up the buccal vestibule while the CT is being performed. This helps to assess the surface of the mucosa that is normally apposed, namely, the cheeks, gingiva, lips, and buccal vestibule. It also helps to predict the extension of the cancer into the buccinator space and retromolar trigone (Fig. 3.6).
The role of the orthopantomogram in assessing contiguous mandibular involvement has diminished with the advent of the CT scan. This is primarily because of a low sensitivity (60% to 64%), high false-positive rates, inability to identify early erosion, and limitation in the region of the middle third of the mandible.
Biopsy
Histopathologic confirmation of malignancy is mandatory and is best established by punch biopsy. This can be performed in the outpatient clinic using a 3- to 5-mm biopsy forceps. Biopsy is targeted from the most representative area avoiding obviously necrotic areas within the lesion. On occasion where punch biopsy is not
feasible (submucosal tumor), an incisional knife biopsy should be performed under local anesthesia. Scrape cytology is not reliable in oral lesions. Whenever clinical suspicion is high and scrape cytology negative, an incisional biopsy is indicated.
feasible (submucosal tumor), an incisional knife biopsy should be performed under local anesthesia. Scrape cytology is not reliable in oral lesions. Whenever clinical suspicion is high and scrape cytology negative, an incisional biopsy is indicated.
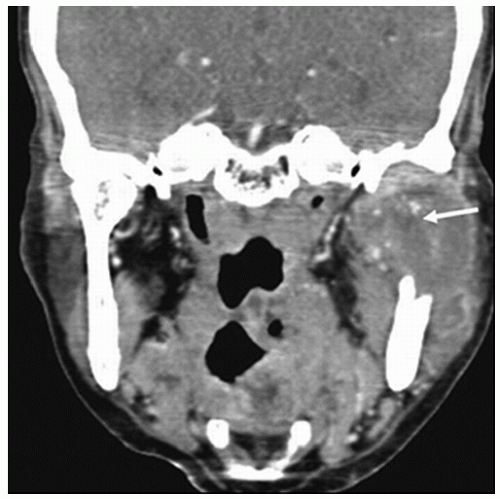 FIGURE 3.5 Coronal CECT reformation demonstrating spread of the cancer into the superior aspect of the infratemporal fossa into the superior aspect of the buccal mucosa (arrow). |
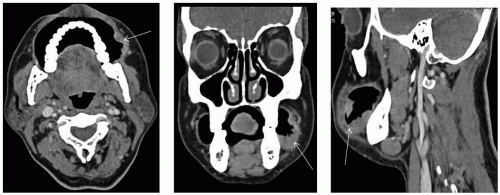 FIGURE 3.6 Axial, coronal, and sagittal CT scan obtained with the puffed cheek technique shows enhancing left buccal buccinator complex mass with involvement of gingivobuccal mucosa (tumor marked by an arrow). |



