Assessment of Pupillary Size, Shape, and Function
Assessment of the pupils requires a precise history and careful examination and may be followed by pharmacologic testing.
History
Patients are often not aware of any abnormality of pupil size. A spouse, friend, or physician may bring the abnormality to attention. The pupil abnormality may be intermittent or episodic. Dating the onset of the pupillary abnormality may be aided by reviewing photographs with the aid of a magnifying lens, although digital photography has made this technique less useful.
Symptoms associated with abnormalities of pupillary size and shape include light sensitivity, difficulty focusing while adjusting to changing lighting conditions, or blurred vision. Complaints of blurry vision are typically nonspecific.
Important past medical history includes a history of previous infections, trauma, operations (particularly in the neck), or migraine. Occupational history may be important. Farmers or gardeners may be exposed to plants or pesticides that produce pupillary dilation or constriction. Physicians, nurses, or other health professionals may work with or have access to topical dilating or constricting substances. Medication history may be important as opiates may cause pupil constriction, and anticholinergics used in inhalers for asthmatics may cause pupillary dilation.
Examination
Slit lamp examination of the anterior segment is essential in patients with a pupillary abnormality. It may reveal a corneal injury that could affect pupillary size or anterior chamber inflammation that may be associated with ciliary spasm and miosis. Examination of the iris should include assessment of the iris sphincter for small traumatic tears and transillumination of the iris for defects. In addition, by placing a wide beam at an angle to the iris and turning the light off and on, the light reflex can be assessed for segmental defects, such as occur in eyes with tonic pupils or aberrant regeneration of the oculomotor nerve.
Pupil measurements may be performed using a hand-held pupil gauge, hand-held pupil camera, or infrared video pupillometry. The hand-held pupil gauge is held next to the eye to determine pupil size in both light and darkness. Pupil gauges consist of a series of solid or open circles or half circles with diameters that increase by 0.2 mm in steps (Fig. 14.1). Infrared video pupillometry is perhaps the most accurate method of assessing the size of the pupil. An infrared video pupillometer permits observation of pupils not only in lighted conditions but also in total darkness. Commercial infrared devices are available and supplant pupil photography but have not been adopted widely.
During clinical evaluation, the examiner should first assess the size of the pupils. The examiner should determine if the pupils are equal. If they are not equal, the examiner should determine whether the difference in size is greater in light or darkness. Other questions that should be answered pertain to whether the pupils constrict with the same velocity, whether they redilate equally with the same velocity, and how the pupillary reaction to light compares to the pupillary reaction to near. Finally, the examiner must assess whether a relative afferent pupillary defect is present.
Assessing Pupillary Size
The diameter of both pupils should be estimated or measured in light, using either normal room light or
a hand-held light source. The diameter of the pupils should then be assessed in darkness, using the dimmest room light in which the examiner can still see the edge of the pupil. Finally, the pupillary size should be assessed during near stimulation using an accommodative target to achieve maximum constriction of the pupils.
a hand-held light source. The diameter of the pupils should then be assessed in darkness, using the dimmest room light in which the examiner can still see the edge of the pupil. Finally, the pupillary size should be assessed during near stimulation using an accommodative target to achieve maximum constriction of the pupils.
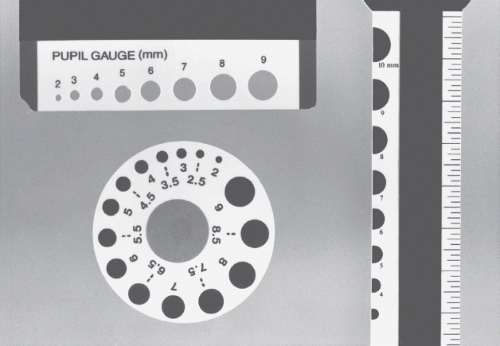 Figure 14.1 Pupil gauges. The best gauges measure in 0.5-mm steps. |
Measurements of the pupil in light and dark should determine if anisocoria, a difference in the pupils of 0.4 mm or more, is present. A substantial percentage (20%) of the normal population has clinically detectable anisocoria, referred to as “physiologic anisocoria.” Anisocoria may be produced by damage to the iris sphincter or dilator muscles or to their nerve supply. The amount of anisocoria may be affected by illumination. For example, a greater degree of anisocoria is present in darkness than in light in patients with physiologic anisocoria or Horner syndrome. Anisocoria can also be affected by the degree of accommodation, by fatigue, and by sympathetic drive.
Testing the Pupillary Reaction to Light
When testing the reaction of a pupil to light shined in the eye—the direct pupillary light reaction—it is important to have a quiet and dimly lit room. The patient must be fixating on a distant target to eliminate any effect of accommodation on pupillary size.
The light source used to illuminate the pupils should be bright enough to produce a maximum rate of constriction and redilation. If the light source is too bright, a prolonged contraction lasting several seconds will occur, making determination of the normal light reflex difficult. It may be helpful to use a dim secondary light source to provide oblique illumination of the pupil in some cases as this technique increases visualization of darkly pigmented irides. Pupil visualization with very dark irides also may be enhanced having the patient look up while the light is directed forward; this technique moves the corneal light reflex away from the axis of the pupil (Fig. 14.2, and Videos 14.1 and 14.2).
The light source should be directed straight into the eye for a few seconds and then moved downward away from the eye to eliminate the stimulation. The pupil response should be assessed during this maneuver, which should be repeated several times. The normal response to a bright light is a contraction called “pupillary capture.” “Pupillary escape,” on the other hand, is a phenomenon in which the pupil initially constricts and then slowly redilates and returns to its original size. Pupillary escape most often occurs on the side of a diseased optic nerve or retina and in normal persons tested with a low-intensity light source. The initial size of the pupil is important in assessing both pupillary capture and pupillary escape. A larger pupil is more likely to show pupillary escape, whereas a smaller pupil is more likely to show pupillary capture.
The latency and speed with which a pupil constricts to light and redilates after light stimulation can be
assessed using pupillography. The use of pupillography to record waveforms of pupillary constriction and dilation is generally limited to research, although commercial pupillographic devices have been developed.
assessed using pupillography. The use of pupillography to record waveforms of pupillary constriction and dilation is generally limited to research, although commercial pupillographic devices have been developed.
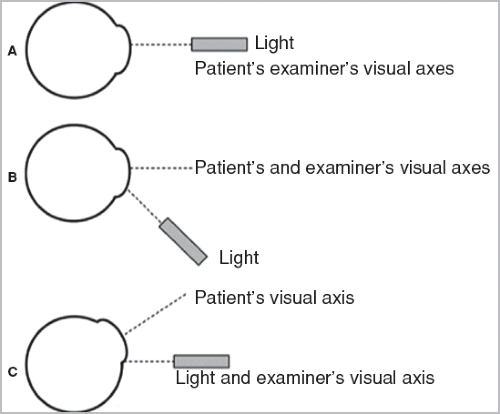 Figure 14.2 Comparison of the oblique illumination technique and upgaze pupil testing technique. A: The normal method of testing the pupillary light reaction is with the patient looking straight ahead and the examiner aiming the light directly at the center of the cornea. B: One way to try to see the pupillary light reaction better in a patient with dark irides is to have the patient look straight ahead and aim the light upward from below. C: An even better way to see the pupillary light reaction in a patient with dark irides is to have the patient look up and shine the light from directly in front of the patient. (Reprinted with permission from Hsu JL, Weikert MP, Foroozan R. Modified upgaze technique for pupil examination. J Neuroophthalmol. 2010;30(4):344–346.) See also videos 14.1 and 14.2. |
When light is shined in one eye, the contralateral pupil constricts as well in a consensual light response. The consensual light response is assessed using a light source for illumination of the pupil of one eye and a dimmer light source that is held obliquely to the side of the contralateral eye being observed. The consensual pupillary response should be approximately equal in both velocity and extent to the direct response, because the pupillary decussation in the midbrain is about 50% to each eye.
Testing the Pupillary Near Response
The near response, a component of the near triad that also includes accommodation and convergence, should be tested in a room with light that is adequate for the patient to fixate an accommodative target. A nonaccommodative target, such as a pencil, may not be a sufficient stimulus to produce a proper near response even in a normal person. The near response should not be induced by having the patient look at a bright light stimulus, because the light itself may produce pupillary constriction. One can document the light and near response with photographs or pupillometry (Fig. 14.3).
Assessment of Pupillary Dilation
Dilation of the pupils occurs in a variety of settings. Most often, the pupils dilate after they have constricted to light or near stimulation. In patients with certain retinal and, less often, optic nerve disease, they may actually dilate when light is shined in one eye (paradoxical pupillary response). Reflex pupillary dilation can also be elicited by sudden noise or by pinching the back of the neck.
When assessing pupillary dilation, the examiner should look specifically for dilation lag. This phenomenon is present when there is more anisocoria 4 to 5 seconds after pupillary constriction to light than there is 15 seconds after pupillary constriction. Dilation lag typically occurs in patients with a defect in the sympathetic innervation of the pupil (i.e., Horner syndrome), although it also occurs in some normal subjects.
Dilation lag may be tested by observing both pupils simultaneously in a very dim light after a bright light
has been turned off. Normal pupils return to their widest size within 12 to 15 seconds, with most of their dilation occurring in the first 5 seconds. Pupils that show dilation lag may take up to 25 seconds to return to maximum size in darkness with most of the dilation occurring about 10 to 12 seconds after the light goes out. Infrared pupillography may help identify the phenomenon as well, although some systems allow only one eye to be viewed at a time.
has been turned off. Normal pupils return to their widest size within 12 to 15 seconds, with most of their dilation occurring in the first 5 seconds. Pupils that show dilation lag may take up to 25 seconds to return to maximum size in darkness with most of the dilation occurring about 10 to 12 seconds after the light goes out. Infrared pupillography may help identify the phenomenon as well, although some systems allow only one eye to be viewed at a time.
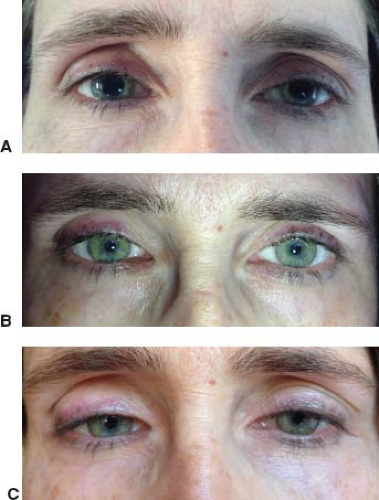 Figure 14.3 Use of a smartphone camera to document size of the pupils in light and darkness in a normal subject. A: In room light without any other stimulation. B: In room light during stimulation with a bright light. C: In room light during stimulation with an accommodative target. Note associated convergence. |
Testing for Light-Near Dissociation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


