History
A careful history should always precede a complete examination of the ocular motor system. Patients with ocular motor disorders may complain of a number of visual difficulties, including diplopia, visual confusion, blurred vision, and the vestibular symptoms of vertigo, oscillopsia, or tilt.
Diplopia
Because misalignment of the visual axes causes the image of an object of interest to fall on noncorresponding parts of the two retinas, usually the fovea of one eye and extrafoveal retina of the other eye, a sensory phenomenon occurs that is usually interpreted as diplopia, the visualization of an object in two different spatial locations. Diplopia may be horizontal, vertical, torsional, or a combination of these.
Diplopia that results from ocular misalignment disappears with either eye closed—it is a binocular phenomenon. Binocular diplopia is almost never caused by intraocular disease, although it may occur in rare patients in the setting of a monocular macular lesion, such as a subretinal neovascular membrane or epiretinal membrane formation. The pathophysiology of binocular diplopia with uniocular disease may represent the establishment of rivalry between central and peripheral fusion mechanisms, as seen in the dragged fovea diplopia syndrome.
Diplopia that persists with one eye closed, monocular diplopia, is rarely caused by neurologic disease. In almost all cases, it is produced by local ocular phenomena, including uncorrected astigmatism or other refractive errors, corneal and iris abnormalities, cataract, and macular disease. Most patients with this type of monocular diplopia recognize a difference in the intensity of the two images that they see and may be described as a “ghost image” that overlaps the clear image. A pinhole will typically eliminate this form of diplopia, making it a useful test in patients suspected of monocular diplopia due to anterior segment or refractive abnormalities.
Cases of monocular diplopia and polyopia are occasionally reported in patients with central nervous system (CNS) disease. Patients with “cerebral polyopia” generally see each image with equal clarity and many copies of the same image. In addition, the monocular diplopia in these patients is always seen with either eye covered. Such patients usually have lesions in the parieto-occipital region and associated visual field defects. The mechanism of cerebral diplopia–polyopia is unknown.
For patients with true binocular diplopia, the eyes are presumably misaligned, and the examiner should ascertain if the diplopia is horizontal, vertical, or oblique; better or worse in any particular direction of gaze; intermittent or constant; different when viewing at distance or near; or affected by head posture.
Visual Confusion
In patients with misalignment of the visual axes, the maculae of the two eyes are simultaneously viewing two different objects or areas, interpreted as existing at the same point in space. This sensory phenomenon is called visual confusion. Patients with visual confusion complain that the images of objects of interest are superimposed on inappropriate backgrounds.
Blurred Vision
Misalignment of the visual axes does not always produce diplopia or visual confusion. In some patients, the images of an object seen by noncorresponding parts of the retina are so close together that the patient
does not recognize two distinctly separated images but instead complains that the vision is blurred when both eyes are open. In such patients, the blurred vision clears completely if either eye is closed.
does not recognize two distinctly separated images but instead complains that the vision is blurred when both eyes are open. In such patients, the blurred vision clears completely if either eye is closed.
Blurred vision that resolves with one but not either eye closed usually suggests a primary visual sensory disturbance. Blurred vision that does not resolve with either eye closed also usually occurs from visual sensory disease but may also occur in some patients with oscillopsia, disorders of saccades (e.g., saccadic oscillations such as ocular flutter), and in patients with impaired pursuit leading to disordered tracking.
Vestibular Symptoms: Vertigo, Oscillopsia, and Tilt
Patients with disorders that affect the vestibular system may complain of disequilibrium or unsteadiness, symptoms that reflect imbalance of vestibular tone. A common complaint of patients with vestibular imbalance (disease of vestibular organ, nerve, or brainstem nuclei) is vertigo, the illusory sensation of motion of self or of the environment. Vertigo usually reflects a mismatch among vestibular, visual, and somatosensory inputs concerning the position or motion of one’s body in space. It is best to evaluate the vestibular sense alone by asking the patient about the perceived direction of self-rotation with the eyes closed, thus eliminating conflicting visual stimuli.
Oscillopsia is an illusory to-and-fro movement of the environment that may be horizontal, vertical, torsional, or a combination of these directions, caused by an instability of fixation, typically of neurologic origin. When oscillopsia is produced or accentuated by head movement it is usually due to vestibular imbalance. Oscillopsia is rarely present when ocular motor dysfunction is congenital (e.g., congenital or latent nystagmus).
A third group of vestibular symptoms include the perception of tilt: static rotation of the perceived world or the body. These complaints usually reflect a disturbance of the otolith organs from either peripheral or central causes. When dealing with such patients, as with patients who complain of vertigo, the examiner should ask about the perception of the position of the body relative to the earth vertical, with the eyes closed to eliminate conflicting visual stimuli.
Examination
The examination of the ocular motor system generally consists of the assessment of (1) fixation and gaze-holding ability, (2) range of monocular and binocular eye movements, (3) ocular alignment, and (4) performance of versions (saccades, pursuit). In addition, depending on the findings of the basic examination, it may be appropriate to test the vestibulo-ocular and optokinetic reflexes to differentiate between supranuclear and nuclear or infranuclear disorders.
Fixation and Gaze-Holding Ability
Principles
In a normal, awake person, the eyes are never absolutely still. Fixation is interrupted by three distinctive types of miniature eye movements including microsaccades, continuous microdrift, and microtremor. Square-wave jerks—spontaneous, horizontal saccades of about 0.5 degrees, followed about 200 msec later by a corrective saccade and occurring at a rate of less than 9 per minute—can also be observed during fixation in most normal individuals.
When no efforts are being made toward ocular fixation or accommodation, the eyes are said to be in a “physiologic” position of rest. With total ophthalmoplegia, there is usually a slight divergence of the visual axes, and this position usually also occurs during sleep, deep anesthesia, and death.
Technique
In patients complaining of intermittent diplopia, visual confusion, or strabismus, tests of sensory fusion (e.g., stereoacuity) and fixation should be performed before the eyes are dissociated by tests of monocular visual function (e.g., visual acuity, color vision, visual fields).
Range of Eye Movements
Principles
To discuss eye movements, it is necessary to have a frame of reference against which any movement may be quantified. Accordingly, the primary position of the eyes is arbitrarily designated as that position from which all other ocular movements are initiated or measured.
All movements of the globe around the hypothetical center of rotation can be analyzed in terms of a coordinate system with three axes perpendicular to each other and intersecting at the center of rotation (Fig. 16.1). The Y axis is equivalent to the visual axis; the Z axis is vertical (around which the eye rotates horizontally); and the X axis is horizontal (around which the eye rotates vertically).
Rotations of either eye alone without attention to the movements of the other eye are called ductions. Horizontal rotation is termed adduction if the anterior pole of the eye is rotated nasally and abduction if the anterior pole of the eye is rotated temporally. Vertical rotation is called elevation if the anterior pole of the eye rotates upward and depression if it rotates downward.
Rotation around either the horizontal or vertical axis places the eye in a secondary position of gaze. In achieving this position, there is no rotation of the globe around the Y axis (i.e., there is no torsion). The
oblique positions of gaze are called tertiary positions. They are achieved by a simultaneous rotation around the horizontal and vertical axes. When an eye moves obliquely out of primary position, the vertical axis of the globe tilts with respect to the X and Z axes.
oblique positions of gaze are called tertiary positions. They are achieved by a simultaneous rotation around the horizontal and vertical axes. When an eye moves obliquely out of primary position, the vertical axis of the globe tilts with respect to the X and Z axes.
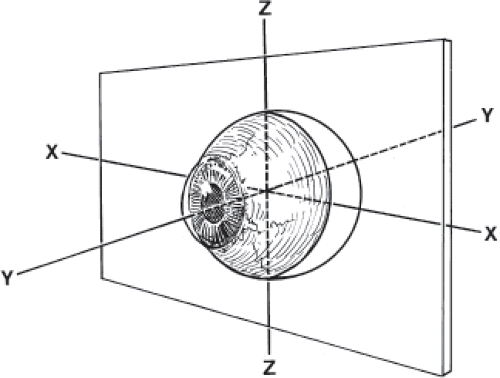 Figure 16.1 The axes of rotation of the eye. The Y axis corresponds to the line of sight when the eye is in the primary position, looking straight ahead. |
True ocular torsion is defined by the direction of the rotation around the Y axis (i.e., the visual axis) relative to the nose. If the 12 o’clock region of the limbus rotates toward the nose, the movement is called intorsion (incycloduction; incyclotorsion). If the same area rotates away from the nose, the movement is called extorsion (excycloduction; excyclotorsion).
Torsion occurs mainly as part of the involuntary compensatory eye movements that take place during head tilt. In this setting, the torsion movements are called countertorsion or counter rolling. Dynamic countertorsion occurs during head tilt and reflects the semicircular canal-induced torsional vestibulo-ocular reflex (VOR). Static countertorsion persists at a given angle of any head tilt, but the amount of rotation is minor compared with that which occurs from dynamic countertorsion. Static countertorsion reflects a tonic otolith–ocular reflex. Each utricle influences both eyes in both directions but primarily controls tilt to the contralateral side.
The actions of the extraocular muscles are typically discussed in terms of individual antagonist pairs and have primary, and potentially secondary, and tertiary actions (see Table 16.1). Normal eye movements are binocular. Such movements are called versions if the movements of the two eyes are in the same direction and vergence movements if they are in opposite directions (i.e., divergence or convergence). For practical purposes, the extraocular muscles of each eye work in pairs during both versions and vergence movements, with one muscle of each eye contracting (the agonist) while its opposing muscle relaxes (the antagonist). The three agonist–antagonist muscle pairs for each eye are the medial and lateral rectus muscles, the superior and inferior rectus muscles, and the superior and inferior oblique muscles. Whenever an agonist muscle receives a neural impulse to contract, an equivalent inhibitory impulse is sent to the motor neurons supplying the antagonist muscle so that it will relax. This is called Sherrington law of reciprocal innervation.
For the eyes to move together to produce a horizontal version, the lateral rectus of one eye and the medial rectus of the opposite eye must contract together. These muscles constitute a yoke pair. The other two yoke pairs are the superior rectus muscle of one eye and the inferior oblique muscle of the other eye, and the superior oblique muscle of one eye and the inferior rectus muscle of the other eye. Implicit in the concept of a yoke pair is that such muscles receive equal innervation so that the eyes move together, which forms the basis of Hering law of motor correspondence.
Table 16.1 Actions of the Extraocular Muscles | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Techniques
When testing the range of ocular movement, the examiner should ask the patient to follow a target through the full range of movement, including the cardinal (or diagnostic) positions of gaze. The eyes are tested individually with one eye covered and together with both eyes open. The normal range of movements
is fairly stable throughout life for all directions except upgaze. Normal abduction is usually 50 degrees; adduction, 50 degrees; and depression, 45 degrees. Limitation of upward gaze in an older individual may simply be age-related and not necessarily a new, pathologic process.
is fairly stable throughout life for all directions except upgaze. Normal abduction is usually 50 degrees; adduction, 50 degrees; and depression, 45 degrees. Limitation of upward gaze in an older individual may simply be age-related and not necessarily a new, pathologic process.
When the range of motion is limited, it is necessary to determine if the limitation is mechanical, and if not, whether the disturbance is supranuclear or peripheral.
Several tests may be used to determine if a mechanical restriction of ocular motion is present. Mechanical limitation of motion (such as that seen in patients with thyroid ophthalmopathy or orbital floor fracture with entrapment) can be inferred if intraocular pressure increases substantially when the patient attempts to look in the direction of gaze limitation.
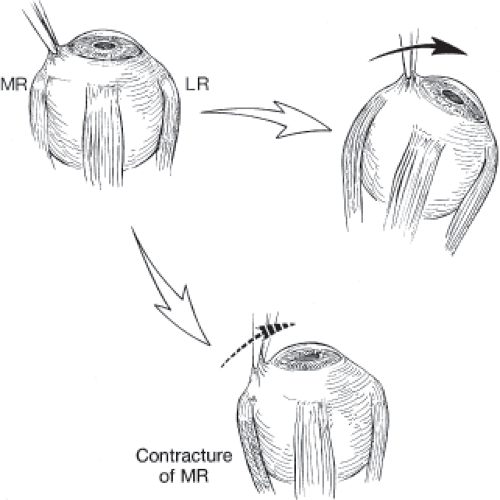
Mechanical limitation of motion can more reliably be detected with forced duction testing. In such tests, an attempt is made to move the eye forcibly in the direction(s) of gaze limitation while the patient is attempting to look in that direction (Fig. 16.2). After adequate topical anesthesia, the conjunctiva is grasped with a fine-toothed forceps near the limbus on the side opposite the direction in which the eye is to be moved. The patient is instructed to try to look in the direction of limitation, and an attempt is made to move the eye in that direction. If no resistance is encountered, the motility defect is not restrictive; however, if resistance is encountered, then mechanical restriction exists. In children or when testing restriction of the oblique muscles, forced duction test can be performed only under general anesthesia.
 Get Clinical Tree app for offline access 
|


