Chapter 31
EVISCERATION AND ENUCLEATION

Following severe injury, several scenarios are possible:
• the eye may be impossible to reconstruct anatomically (A);
• SO may develop (B);
• the eye with no hope of functioning may have a higher than usual risk of developing SO (C);
• unbearable chronic pain may develop in a blind eye and other methods to alleviate it may prove unsuccessful or are not recommended (D);
• the eye may become phthisical and cosmetically unacceptable (E).
In case of “A,” primary enucleation or evisceration is the only reasonable option; in case of “B” (see Chapter 29), it is controversial whether any, and if so which, of the potential procedures discussed in this chapter should be performed; in cases of “C” through “E,” the ophthalmologist must thoroughly discuss all surgical and nonsurgical management options with the patient (see Chapters 5, 7, and 8).
DECISION MAKINGa
Treatment options for painful, blind, and cosmetically unappealing eyes include:
• retrobulbar alcohol injection;
• cyclocryopexy (these two measures usually:
 ruin the motility of a subsequently implanted prosthesis;
ruin the motility of a subsequently implanted prosthesis;
 create moderate to severe ptosis;
create moderate to severe ptosis;
 create sulcus retraction secondary to fat atrophy; and
create sulcus retraction secondary to fat atrophy; and
 have an effect that is temporary and unpredictable);
have an effect that is temporary and unpredictable);
• evisceration; and
• enucleation.
if it is decided that the eye is best removed (see Chapter 8), the selection between evisceration and enucleation is primarily determined by:
• the expertise of the operating physician;
• the implant materials available; and
• the fear of SO development.
Extensive counseling is always required (see later in this chapter and Chapters 5 and 7).
PEARL… The ophthalmologist should always explain that the patient will be fitted with a prosthesis 6 to 8 weeks postoperatively and that a patch may be needed in the interim.
SO AS A FACTOR IN DETERMINING THE MANAGEMENT
The fear of the fellow eye’s involvement (see Chapter 29) and subsequent contralateral blindness are the main reason why some ophthalmologists are reluctant to recommend evisceration. The causal relationship between evisceration and SO has been debated since the 19th century. The conclusion of a literature review1 of 1628 cases in 1963 argued against the role of evisceration as the cause of SO and recommended that evisceration, rather than enucleation, be offered to patients, unless:
• chronic inflammation is present; or
• malignancy cannot be excluded and pathologic examination is required.
It appears that this recommendation has been upheld,b especially because in a series of 105 cases of SO,3 no eye was found to have undergone evisceration.c Furthermore, in cases of severe orbital and ocular trauma, particularly when there are a large posterior scleral rupture and extrusion of intraocular contents into the orbit, the only way to be certain that the threat of SO has been eliminated would be to remove all potential antigens. In this setting, one can reasonably argue that enucleation offers no theoretical benefit over evisceration.
CONTROVERSY
With the increasing threat of litigation, one cannot avoid the question: is it indeed safe to recommend evisceration rather than enucleation?1–5
EVISCERATION
Because the sclera is retained and the extraocular muscle attachments are preserved, evisceration is usually considered to result in:
• superior motility;
• less implant migration;
• less severe manifestation of the anophthalmic socket syndrome; and
• a more physiologic solution for the orbit’s long-term health (Fig. 31–1).
In addition, most ocularists until recently preferred fitting eviscerated sockets compared with enucleated sockets. patients are also more gratified with the overall cosmetic results and motility after evisceration than after enucleation (Figs. 31–2 through 31–4).

FIGURE 31–1 A 73-year-old patient showing classical signs of anophthalmic socket syndrome including hollowing of supratarsal sulcus, downward angulation of lateral canthus, and laxity of right lower lid. This patient had a quasi-integrated buried implant but nevertheless poor motility. The manifestations of the anophthalmic syndrome as depicted here are to be avoided.
Indications
Local and systemic factors alike may require the eye to be eviscerated rather than enucleated:
• posterior scleral rupture without hope of visual rehabilitationd; and
• debilitated patient too sick for general anesthesia and enucleation.
Surgical Technique
Evisceration without Keratectomy
See Figure 31–7A–C.
• Make a limbal periotomy or conjunctival incision 8 to 9 mm from the limbus over the superior 100 degrees of the globe and expose the superior rectus muscle insertion.
• Weave a double-armed suture of 6–0 Vicryl through the superior rectus insertion and “whip-lock” it on each end.
• Divide the superior rectus fascial attachments, detach the superior rectus, and tag the suture with a serrefine on a “mosquito” hemostat.
• Perform a “scratch-down” sclerotomy posterior, temporal, and nasal to the superior rectus insertion over the superior 100 degrees, but do not penetrate the choroid.
• Insert a cyclodialysis spatula to separate the potential space between the adherent anterior uveal attachments and the scleral spur. Once the correct plane is entered, avoid piercing the vitreous cavity by making small initial sweeps with the spatula hugging the sclera.

FIGURE 31–2 This 4-year-old patient suffered posterior scleral laceration and optic nerve avulsion and underwent primary evisceration with a 18-mm hydroxyapatite implant. Three months postoperatively, a beautiful socket is seen with deep fornices and almost no manifestations of the anophthalmic syndrome.

FIGURE 31–3 Same patient as shown in Figure 31–2. Eviscerated socket even without pegs has a good range of motility but not saccadic eye movement (left gaze).

FIGURE 31–4 Same patient as in Figures 31–2 and 31–3, showing right gaze with fair motility of the eviscerated left socket without motility peg.
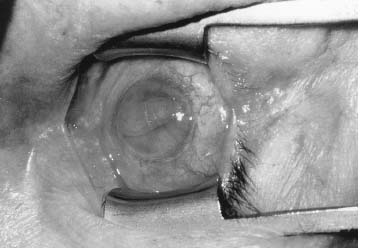
FIGURE 31–5 Pre-enucleation photograph of the right eye of the 69-year-old patient who underwent unsuccessful retinal detachment repair due to advanced PVR. Subsequently, nuclear sclerosis developed in her left eye; 4 years after cataract surgery and 12 years after unsuccessful retinal detachment repair in the right eye, she developed severe uveitis. The enucleated specimen demonstrated sympathetic uveitis. Despite treatment with topical periocular injections of steroids as well as oral steroids and treatment for 3 years with cyclosporine, the visual acuity in the left eye deteriorated from 20/20 to NLP and the eye is now phthisical. (The picture was reversed during processing from a color slide to a black and white print.)
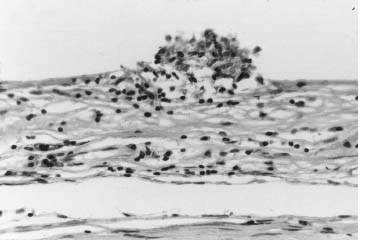
FIGURE 31–6 Pathologic specimen taken from the enucleated right eye of patient in Figure 31–5. Photomicrograph demonstrates Dalen-Fuchs nodule.
• Make larger sweeps in all directions as more choroid is separated until the dissection has covered a full 360 degrees from the sclerotomy. These maneuvers are easier if the globe is normotensive. In open globes or chronically-inflammed eyes, dissection is more difficult and bleeding can be profuse. In such eyes and even with the most deliberate and meticulous initial technique, small pieces of the uvea will most likely remain attached to the sclera; these must be retrieved later.
• Once the cyclodialysis spatula has initiated the dissection, extend the scleral incision and insert a small evisceration spoon to separate the remaining uveal attachments from the sclera. Fixation of a hypotonus globe with forceps by an assistant is helpful. Keep the blade of the spoon angled firmly against the sclera during scraping. Most of the posterior dissection with the evisceration spoon is done by “feel” because the surgical field is bloody and the sclera “floppy.”
• When the uvea is completely dissected, the specimen should be delivered in toto, i.e., including choroid, retina, vitreous, and lens (if present). Positioning the large evisceration spoon around the back of the specimen and scooping it out from behind “in one fell swoop” facilitates this maneuver. The profuse bleeding that usually occurs from the severed central retinal artery may be controlled via:
 application of direct finger pressure over the optic nerve for 5 minutes;
application of direct finger pressure over the optic nerve for 5 minutes;
 cauterizing the optic nerve ab interno with bipo-lar cautery; or
cauterizing the optic nerve ab interno with bipo-lar cautery; or
 Bovie cautery suction if necessary for visualization; alternatively, insert a hemostat through the sclerotomy and clamp the area of the optic disk directly. The clamp may be either left in place for 3 to 5 minutes or immediately electrocoagulated with a Bovie cautery.
Bovie cautery suction if necessary for visualization; alternatively, insert a hemostat through the sclerotomy and clamp the area of the optic disk directly. The clamp may be either left in place for 3 to 5 minutes or immediately electrocoagulated with a Bovie cautery.
• Once the field is bloodless, remove any retained uveal fragments with gauze “peanuts” tightly clamped to hemostats.
• Scrape off the corneal endothelium with absolute alcohol or iodine on a cotton-tipped applicator.
• Irrigate the scleral cavity with hydrogen peroxide, removing uveal cells and intracellular debris.
• Irrigate the scleral cavity with an antibiotic solution (e.g., bacitracin).
• Close the sclera and conjunctiva with multiple interrupted sutures of 4–0 Vicryl.
• Reattach the superior rectus to its original insertion anterior to the scleral incision with 6–0 Vicryl.
• Suture the conjunctiva to the limbus with 6–0 chromic gut.
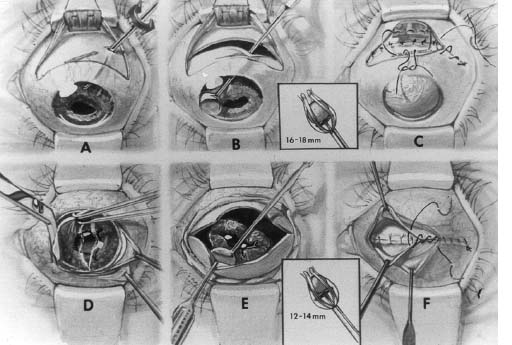
FIGURE 31–7 Technique of evisceration. (A-C) Without keratectomy. (D-F) With keratectomy. (From Callahan MA, Callahan A. Removal of eye. In: Ophthalmic Plastic and Orbital Surgery. Birmingham: Aesculapius Publishing Company. 1979, 43. Reprinted by permission from the Aesculapius Publishing Company, Birmingham, Alabama.)
Evisceration with Keratectomy
See Figure 31–7D-F.e
• Perform a 360–degree limbal peritomy of the conjunctiva and Tenon’s capsule, and remove the cornea with corneoscleral scissors. This is facilitated if the assistant fixates the globe by:
 directly grasping the sclera or
directly grasping the sclera or
 using bridle sutures to hold the superior and inferior rectus muscles.
using bridle sutures to hold the superior and inferior rectus muscles.
• Separate the conjunctiva from Tenon’s capsule for a distance of 8 to 10 mm.f
• After removing the cornea, core out the attachments of the uvea to the sclera with the cyclodialysis spatula and evisceration spoon. As described previously, use initial small spoon sweeps, progressing to larger ones shearing the uvea off the sclera, ideally in a single piece.
• After the specimen is delivered, stop the bleeding as described previously.
• Inspect the inside of the sclera for any uveal remnants. Scrape them off with an evisceration spoon, curette, or gauze stretched tightly over your finger, or use peanuts.
• Excise small triangles at the edge of the sclera at 3 and 9 o’clock, converting the defect into more of an ellipse, so the sclera may be coated tightly without dog ears (inset).
• Insert an 18-mm hydroxyapatite “baseball” implant.
 Alternatively, a 20-mm hydroxyapatite implant may be inserted by making two to four transscleral posterior relaxing incisions 3 mm in length with a Bard-Parker No. 15 blade or Colorado straight needleg between the muscle insertions to allow the sclera to “bow” posteriorly. (A 360–degree ab interno posterior sclerectomy around the optic nerve to detach it can be combined with the above.)
Alternatively, a 20-mm hydroxyapatite implant may be inserted by making two to four transscleral posterior relaxing incisions 3 mm in length with a Bard-Parker No. 15 blade or Colorado straight needleg between the muscle insertions to allow the sclera to “bow” posteriorly. (A 360–degree ab interno posterior sclerectomy around the optic nerve to detach it can be combined with the above.)
• Once the implant is inserted, irrigate the cavity with an antibiotic solution.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


