Purpose
To evaluate United States Public Health Service (USPHS) guidelines for discontinuing anticytomegalovirus (CMV) therapy in patients with AIDS who have immune recovery and quiescent retinitis after initiating highly active antiretroviral therapy.
Design
Cohort study of patients with CMV retinitis (Longitudinal Study of Ocular Complications of AIDS).
Methods
Participants had CMV retinitis and CD4+ T-cell counts of 50 cells/μL or fewer enrolled from 1998 through 2009 who demonstrated sustained immune recovery (2 consecutive CD4+ T-cell counts of 100 cells/μL or more at least 6 months apart) and inactive retinitis. Participants were classified into 2 groups according to anti-CMV treatment after immune recover: (1) continued anti-CMV therapy and (2) discontinued therapy. We evaluated survival, visual acuity, and CMV retinitis activity; we used propensity scores to adjust for confounding factors for these analyses.
Results
Of 152 participants reviewed, 71 demonstrated immune recovery, 37 of whom discontinued therapy and 34 of whom continued therapy. At immune recovery, participants continuing therapy tended to be older (44 vs 40 years; P = .09), have bilateral retinitis (53% vs 32%; P = .10), and have lower CD4+ T-cell counts (148 vs 207 cells/μL; P < .001). There were no statistical differences in any of the clinical outcomes (death, retinitis progress, visual acuity, or incidence of bilateral retinitis). Both groups lost visual acuity during follow-up, on average 1.2 letters per year ( P < .01).
Conclusions
Discontinuation of anti-CMV therapy after immune recovery did not increase the risk of poor outcomes. These results support the current guidelines for discontinuation of anti-CMV therapy after achievement of sustained immune recovery.
Cytomegalovirus (CMV) retinitis typically is a late-stage opportunistic infection in patients with AIDS and severe immunodeficiency (CD4+ T-cell counts of fewer than 50 cells/μL). Before the introduction of highly active antiretroviral therapy (HAART), cytomegalovirus (CMV) retinitis developed in up to 30% of patients with AIDS. Chronic maintenance therapy with an anti-CMV agent was required to prevent reactivation of the disease; time to retinitis progression after stopping therapy typically was 6 to 8 weeks. After the introduction of HAART, the incidence of CMV retinitis declined dramatically because of the preservation or restoration of immune function in many patients with AIDS associated with the use of HAART. There have been several case reports of patients with AIDS-related CMV retinitis who experience immune recovery, as evidenced by a sustained increase in CD4+ T cell counts to more than 100 cells/μL, reporting that they can discontinue maintenance therapy without reactivation of CMV retinitis. There have not been long-term studies comparing survival and vision loss in patients discontinuing treatment with those continuing treatment after immune recovery.
Based on the case reports of successful discontinuation of treatment without disease reactivation, the United States Public Health Service (USPHS) guidelines for secondary prophylaxis were revised in 1999 to suggest discontinuing anti-CMV therapy after patients with quiescent retinitis achieve sustained immune recovery. Continued close follow-up by an ophthalmologist is recommended because reactivation of retinitis and vision loss as a result of CMV retinitis may occur among patients with CD4+ T-cell counts higher than 200 cells/μL, albeit at much reduced rates. The purpose of this analysis was to evaluate and compare clinical outcomes (retinitis activity, visual acuity loss, and survival) between patients who continued with maintenance anti-CMV therapy after immune restoration compared with those who discontinued therapy according to the USPHS treatment guidelines. Participants with CMV retinitis enrolled and followed up in the multicenter Longitudinal Study of Ocular Complications of AIDS between 1998 and 2009 were evaluated.
Methods
The longitudinal study of ocular complications of AIDS is a prospective, observational study designed to collect data on the incidence, prevalence, and complications resulting from AIDS-related ocular morbidities during the era of HAART. Recruitment began in 1998 at 19 clinical centers across the United States, most located in urban areas with large HIV-infected populations. The study is an open-cohort design, and recruitment is continuing at least through 2011. The protocol and consent statements were approved by institutional review boards at all participating centers. Eligible patients were diagnosed with AIDS as defined by the 1993 Centers for Disease Control diagnostic criteria for AIDS. Participants eligible for this analysis were enrolled from September 1998 to January 2009; the data base was frozen for this analysis as of July 31, 2009.
Participants with CMV retinitis were seen every 3 months for the first 10 years of the study (September 1998 through July 2008), after which they were seen every 6 months (August 2008 through July 2009). At each follow-up visit, participants underwent an eye examination that included slit-lamp examination and dilated indirect ophthalmoscopy, a medical history interview, and assessment of best-corrected visual acuity using logarithmic visual acuity charts according to a standard protocol. The location of the CMV retinitis lesion in each eye was categorized into 3 zones based on a standard classification system. Zone 1 is defined as the area within 1500 μm of the optic nerve or within 3000 μm of the center of the macula. Zone 2 extends from zone 1 to the vortex veins, and zone 3 lies anterior to the vortex veins. Immune recovery uveitis was diagnosed clinically as the presence of intraocular inflammation in a patient who had undergone immune recovery. Laboratory tests obtained at each follow-up visit included hematology, lymphocyte subset analysis, and HIV viral load determinations. Participants meeting the eligibility requirements described below were included in this analysis.
Eligible participants were those with a diagnosis of CMV retinitis at enrollment or during follow-up receiving anti-CMV treatment who had a CD4+ T-cell count of 50 cells/μL or fewer who were observed to have immune recovery during follow-up. Immune recovery was defined as having CD4+ T-cell counts of 100 cells/μL or more at 2 or more consecutive visits at least 6 months apart. The date of immune recovery was set at the date of the second CD4+ T-cell count of 100 cells/μL or more. We classified these participants according to the initial management strategy for maintenance therapy after immune recovery, that is, whether the USPHS recommendation was initiated 6 months after immune recovery or not. Participants with CMV retinitis whose CD4+ T-cell counts were never observed to be fewer than 50 cells/μL were excluded because an approximate date of immune recovery could not be determined.
Characteristics at immune recovery were compared via chi-square or Wilcoxon rank-sum tests for categorical or continuous variable, respectively. We also evaluated mortality, retinitis progression, and changes in visual acuity and compared these outcomes between the groups. Survival outcomes (mortality and retinitis progression) were evaluated with Kaplan-Meir curves and proportional hazards regression models with staggered entry; the entry anchor time (time = 0) was the date of immune recovery (the second consecutive CD4+ T-cell count of 100 cells/μL or more). Analyses needed to be adjusted for confounders because the allocation of patients to discontinue versus continue therapy was not randomized, and therefore was prone to selection bias. Because the number of confounders was large relative to the number of observations, we chose to use propensity scores for covariate adjustment. Hazard ratios were adjusted for the following characteristics measured at the time of immune recovery: gender, CD4+ T-cell counts, age, bilateral disease status, and time since CMV diagnosis; for eye-specific outcomes, the percentage of retina involved with CMV retinitis also was included in the model, and P values were adjusted for patient-level clustering. For visual acuity, we defined time 0 as the date of immune recovery and used general linear models with patient-level clustering to evaluate change in visual acuity over time.
Results
We identified 152 participants with CMV retinitis at study enrollment or incident retinitis that occurred during follow-up who had CD4+ T-cell counts of less than 50 cells/μL and were receiving anti-CMV therapy. Sixty-nine (45%) participants were diagnosed with CMV retinitis before study enrollment, 64 (42%) were diagnosed with CMV retinitis at enrollment, and 19 (13%) were diagnosed during follow-up. Of these 152 participants, 71 (47%) had evidence of immune recovery during follow-up: 38 (55%) with CMV retinitis diagnosed before enrollment, 31 (48%) of those with a new diagnosis at enrollment, and 2 (11%) with incident disease during follow-up. Most of these 71 participants were observed to achieve immune recovery after January 2000 ( Table 1 ). We followed up these participants for a median of 5 years (interquartile range, 3 to 7 years) after immune recovery.
| D/C CMV Rx | Cont. CMV Rx | P Value a | |
|---|---|---|---|
| No. | 37 | 34 | |
| Demographics | |||
| Median age (IQR), y | 40 (35 to 44) | 44 (37 to 49) | .09 |
| Male gender, n (%) | 29 (78%) | 24 (71%) | .59 |
| Race, n (%) | .69 | ||
| White, non-Hispanic | 14 (38%) | 11 (32%) | |
| Black, non-Hispanic | 15 (40%) | 11 (32%) | |
| Hispanic | 6 (16%) | 9 (26%) | |
| Other | 2 (5%) | 3 (9%) | |
| HIV characteristics | |||
| HIV exposure, n (%) | .50 | ||
| Male to male sexual contact | 19 (51%) | 12 (32%) | |
| Injection drug use | 1 (3%) | 2 (6%) | |
| Heterosexual contact | 12 (32%) | 12 (35%) | |
| Other | 5 (14%) | 8 (23%) | |
| HIV viral load ‘ 400 copies/mL, n (%) | 20 (54%) | 18 (53%) | .78 |
| Median CD4 count (IQR), cells/μL | 207 (157 to 295) | 148 (129 to 170) | .001 |
| HAART exposure, n (%) | 31 (84%) | 28 (82%) | 1.00 |
| Antiretroviral treatment category, n (%) | 1.00 | ||
| None | 1 (3%) | 0 (0%) | |
| 1 to 2 therapies | 2 (5%) | 2 (6%) | |
| HAART without protease inhibitor | 27 (73%) | 25 (74%) | |
| HAART with protease inhibitor | 4 (11%) | 3 (9%) | |
| Date achieved immune recovery | .29 | ||
| Before January 2000 | 6 (16%) | 2 (6%) | |
| January 2000 through December 2004 | 24 (65%) | 22 (65%) | |
| January 2005 or later | 7 (19%) | 10 (29%) | |
| CMV retinitis characteristics | |||
| Bilateral involvement, n (%) | 12 (32%) | 18 (53%) | .10 |
| Median duration from CMVR Dx to CD4 recovery (IQR), y | 2.4 (1.1 to 4.3) | 1.5 (0.9 to 3.7) | .15 |
| Median follow-up (IQR), y b | 6.4 (3.3 to 8.1) | 4.5 (3.0 to 6.4) | .16 |
a Based on Fisher exact test for categorical variables and Wilcoxon rank-sum test for measured variables.
Thirty-seven of the eligible participants (52%) discontinued anti-CMV treatment within 6 months of achieving immune recovery, and the remaining 34 patients continued to receive anti-CMV therapy for more than 6 months after immune recovery ( Table 1 ); the median length of continuous therapy was 2.1 years (95% confidence interval, 1.5 to 2.7 years). Participants who continued anti-CMV therapy tended to be older and had lower CD4 counts at the time of immune recovery. More than 80% of participants in both groups were receiving HAART at the time of immune recovery and continued during follow-up (data not shown).
Participants who continued treatment tended to have a higher rate of bilateral disease, despite the fact that they tended to have a shorter duration from their diagnosis of CMV retinitis to immune recovery ( Table 1 ). The median percentage of retinal area involved with retinitis was the same in both groups, and the proportion with involvement of the posterior areas of the retina (zone 1 disease) was similar ( Table 2 ). None of the eyes with CMV retinitis in either group had evidence of CMV lesion border activity at the time of immune recovery. The median visual acuity at immune recovery in eyes with CMV retinitis was less in the eyes of patient’s who discontinued treatment, but the difference was not statistically significant, and both groups had similar levels of visual acuity impairment in involved eyes ( Table 2 ).
| D/C CMV Rx | Cont. CMV Rx | P Value a | |
|---|---|---|---|
| No. eyes with retinitis | 49 | 52 | |
| CMV retinitis | |||
| Percent of retina involved, median (IQR) | 20 (15 to 50) | 20 (10 to 50) | .43 |
| Eyes with zone 1 involvement, n (%) | 17 (35%) | 21 (40%) | .68 |
| Eyes with zone 2 involvement, n (%) | 40 (82%) | 38 (73%) | .35 |
| Eyes with zone 3 involvement, n (%) | 42 (86%) | 36 (69%) | .06 |
| Visual acuity | |||
| Standard letters, median (IQR) | 75 (46 to 86) | 82 (57 to 90) | .31 |
| Worse than 20/40, n (%) | 19 (39%) | 18 (35%) | .66 |
| 20/200 or worse, n (%) | 10 (20%) | 11 (21%) | .93 |
a Based on Fisher exact test for categorical variables and Wilcoxon rank-sum test for measured variables.
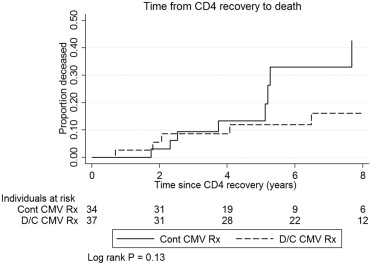
There were no statistically significant differences in the development of bilateral retinitis, mortality, retinitis progression, or visual acuity loss between the groups ( Table 3 ; Figure 1 , Kaplan-Meir curve for mortality). All cases of retinitis progression were associated with a decline in CD4+ T-cell counts to fewer than 100 cells/μL, ranging from 3 to 66 cells/μL.
| No. (Events/100 y) b | Adjusted a | ||||
|---|---|---|---|---|---|
| D/C CMV Rx | Cont. CMV Rx | HR | 95% CI | P Value | |
| Participants | 37 | 34 | |||
| Deceased | 5 (2.2) | 8 (4.8) | 1.71 | 0.41 to 7.22 | .46 |
| Participants c | 25 | 16 | |||
| Incident bilateral retinitis | 3 (1.1) | 4 (1.5) | 2.12 | 0.44 to 10.09 | .35 |
| Eyes with retinitis | 49 | 52 | |||
| CMV retinitis progression | 2 (0.7) | 4 (1.5) | 0.62 | 0.16 to 2.50 | .50 |
| Eyes with retinitis c | 30 | 34 | |||
| Worse than 20/40 | 14 (11.6) | 10 (7.6) | 0.82 | 0.26 to 2.61 | 0.74 |
| Eyes with retinitis c | 39 | 41 | |||
| 20/200 or worse | 9 (4.3) | 5 (2.7) | 0.49 | 0.12 to 2.95 | .53 |
a HR and 95% CIs calculated using Cox models comparing continued CMV treatment with discontinued treatment at immune recovery; CIs and P values corrected for within-patient clustering for visual acuity outcomes. HRs adjusted for the following characteristics measured at immune recovery: CD4 count, log of HIV load, age, gender, bilateral disease status, and years since CMV diagnosis. Eye-specific outcomes also were adjusted for percentage of retinal involvement, and P values were corrected for within-patient clustering. All adjustments were made using propensity scores.
b Rate per 100 person-years of follow-up for death and incidence of bilateral disease; rate per 100 eye-years of follow-up in eyes with retinitis at immune recovery for retinitis progression and visual acuity events.
c Number of patients (or eyes) without event of interest at immune recovery.
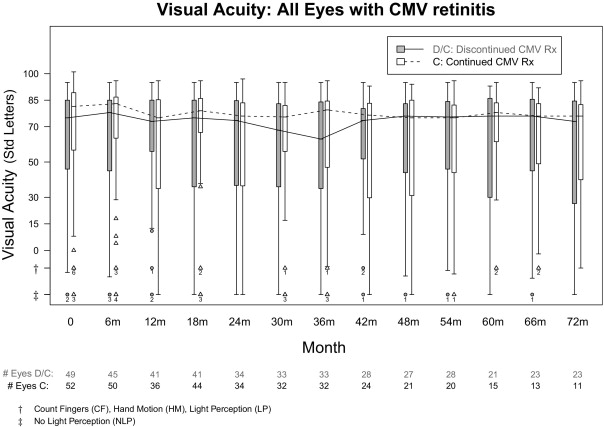
Both groups experienced similar losses of visual acuity overtime at similar rates ( P = .94; Figure 2 ). The overall average rate of loss was 1.2 standard letters per year, which was significantly different from 0 ( P < .01). The rates of visual loss to standard thresholds, that is, worse than 20/40 or 20/200 or worse, were high in both groups ( Table 2 ), with nominally higher rates in the participants discontinuing anti-CMV treatment. However, that group tended to have a lower visual acuity at immune recovery, which may account for this trend.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


