A variety of lesions have been reported to cause facial paralysis; these can be broadly classified as traumatic, idiopathic, toxic, metabolic, infective, neoplastic, and degenerative (1). When confronted with a patient suffering from facial paralysis, the immediate task of the clinician is to uncover the probable cause. According to Sir Terrance Cawthorne (2), “all that palsies is not Bells,” and it is for this reason that a detailed history with respect to the mode of onset, progression of paralysis, and history of head trauma and associated otologic and neurologic symptoms is important. Facial paralysis can be supranuclear or infranuclear. The latter can be unilateral and acute in onset or chronic, progressive in nature. The acute form could also be bilateral (simultaneous or sequential) or ipsilaterally recurrent. The purpose of this chapter is to discuss the evaluation of facial paralysis as it presents to the clinician in any of the forms just described.
ACUTE PALSIES
Bell’s Palsy and Herpes Zoster Oticus
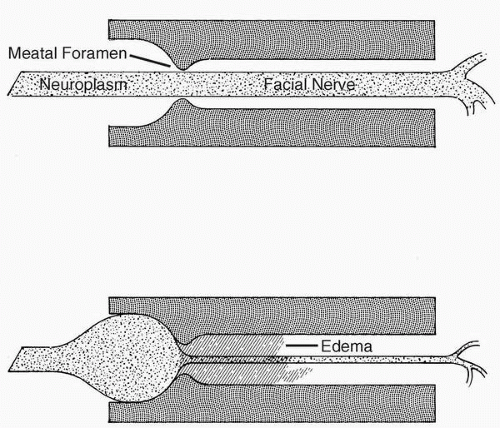
The most common type of acute onset unilateral facial paralysis is Bell’s palsy. The cause of Bell’s palsy has long been held to be idiopathic, and the diagnosis is made by the characteristic clinical features and by a process of exclusion (3). Today, Bell’s palsy is regarded as a neuritis of the nerve within the fallopian canal. Recent studies have demonstrated ample clinical, histopathologic, experimental, imaging, and therapeutic evidence to support a viral infection of the nerve with the herpes simplex type 1 virus (4, 5, 6, 7, 8). The infection produces inflammation and edema of the nerve. Fisch (9) proposed that the neural compression and conduction block occurs at the meatal foramen secondary to nerve edema (Fig. 6.1). He defined the meatal foramen as the medial opening of the fallopian canal into the internal auditory meatus (9). His measurements of the fallopian canal showed that the meatal foramen is its narrowest segment (0.68 mm); he termed it the “bottle-neck.”(9)
Herpes zoster oticus (Ramsay Hunt syndrome), on the other hand, is caused by the varicella zoster virus. The clinical presentation is characterized by vesicles on and around the pinna (3). The clinical evaluation and diagnostic workup are similar to those for Bell’s palsy.
Clinically, two patients may present with an equally dense House-Brackman grade 6 paralysis. One may improve to grade 2, and the other may recover to only grade 5. How can the physician prognosticate the final outcome? Today it is generally accepted that the best method for accurately predicting the final outcome is from the results of serial electrophysiologic tests. The selection of the test most appropriate for a given situation and interpretation of the results will be facilitated by an understanding of the underlying pathologic changes that occur in the facial nerve secondary to injury.
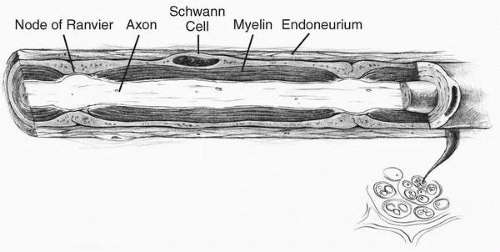
In the facial nerve there are about 10,000 axons, of which 7,000 are branchial motor axons. The rest are afferent taste fibers from the anterior two-thirds of the tongue, as well as efferent parasympathetic secretomotor fibers from the lacrimal, nasal, submandibular, and sublingual glands (10). The structure of each branchial motor axon is similar to that of any peripheral nerve except that the size is different. The axoplasm is surrounded by a myelin sheath, and these myelinated fibers are encased in a connective tissue tubule, the endoneurium (Fig. 6.2). In peripheral nerves, groups of axons are surrounded by concentric sleeves of flattened polygonal cells called perineurium. Each such collection of axons enclosed by perineurium is a fascicle. Peripheral nerves are made up of groups of fascicles, which in turn are held together by a condensation of loose areolar connective tissue, the epineurium. The structure of the facial nerve, however, has been shown to be different from that of peripheral nerves in that the facial nerve has just a single fascicle in its intratemporal course (11,12).
According to the Sunderland (12) classification (Table 6.1), the least severe nerve injury is designated as first degree and in this there is only a physiologic block to propagation of the nerve impulse. The axon, its myelin sheath, and the endoneural tube distal to the labyrinthine segment are intact. This degree of injury had been described earlier by Seddon (13) as neuropraxia. In Bell’s palsy, such an injury results from increased intraneural pressure at the meatal foramen (9). Normal nerve impulses are therefore not conducted across the site of compression and hence the face is paralyzed (Fig. 6.3). However, electrical stimulation of the nerve distally elicits a response because the axoplasm and myelin sheath are intact. If the compression is not relieved, venous drainage is obstructed and intraneural pressure continues to increase. This leads to Sunderland’s second degree injury (12). Seddon (13) called this degree of injury axonotmesis. In this type of injury the axons are destroyed but the endoneural tubules remain intact (Fig. 6.4). Consequently, recovery is prolonged but nerve regeneration is not faulty because the intact endoneural tubes guide the regrowth of the axons. If the majority of axons suffer this degree of injury, synkinesis is an unlikely sequela of recovery.
FIG. 6.1Top figure illustrates normal cross-sectional dimensions of the whole length of the fallopian canal. Bottom figure illustrates the bottle-neck created by the meatal foramen. The nerve is injured at this site because the edematous nerve is constricted within the fallopian canal.
FIG. 6.2 Illustration of the structure of a single myelinated nerve fiber.
The pathologic process in Bell’s palsy and herpes zoster oticus usually does not progress past Sunderland’s second-degree injury (axonotmesis). The majority of patients with Bell’s palsy must suffer this degree of injury because Peitersen observed that 71% of patients with untreated Bell’s palsy recovered without any sequelae in a cohort of 1,011 patients (14). With continued increase in intraneural pressure, Sunderland’s third and fourth degree injuries may occur. With these degrees of nerve damage, there is axolysis, disruption of the myelin sheath, and loss of endoneurial tubes. The percentage of responding fibers progressively reduced with time, and the graph shown in Figure 6.5 represents these surviving axons. If by the sixth day there are no stimulatable axons (i.e., neuropraxic and surviving fibers), the prognosis for good recovery is poor. In addition, with loss of endoneurial continuity, there is a potential for mismatching of branchial motor and secretomotor fibers during regrowth, resulting in the clinical observation of synkinesis and crocodile tears in grade 3 and 4 injuries. Furthermore, with time, considerable intraneural fibrosis ensues, blocking axonal regrowth. Though both these grades of injury may occur in a case of Bell’s palsy, a relatively small number of patients are so affected. Peitersen’s (14) study is illustrative because only 16% of untreated Bell’s palsy patients showed a poor recovery of function. It is important to note that the various degrees of injury can overlap in any patient with Bell’s palsy. Complete or partial nerve transection was described by Sunderland (12) as fifth degree injury (Seddon’s neurotmesis [13]), but such an injury does not occur in Bell’s palsy. Transection is more likely with blunt head trauma, penetrating ear trauma, or trauma during the course of surgery.
Interruption of the axon leads to early retrograde changes in the nerve cell body and the nerve proximal to the site of injury. Anterograde changes in the nerve distal to the site of injury begin within 12 hours of the insult. These anterograde changes are called Wallerian degeneration. The axoplasm is destroyed and the myelin sheath disintegrates and is phagocytized by activated macrophages. The Schwann cells proliferate and form the bands of Bunger, which fill the endoneural tubes if these are intact. The bands of Bunger strongly support axonal regeneration. In most instances, Wallerian degeneration is complete by 12 to 14 days after injury. Regenerated nerves have thinner myelin and the distance between the nodes of Ranvier are altered (11). As a result, nerve conduction velocity is slowed and there is an increase in the threshold for depolarization. It is for this reason that electroneurography (ENoG) has no value in a regenerating nerve.