Purpose
To evaluate the efficacy of a thermosensitive atelocollagen punctal plug in the treatment of dry eye disease.
Design
Prospective observational case series.
Methods
The thermosensitive atelocollagen punctal plug was warmed at 37 C, 39 C, 41 C, and 43 C to evaluate the appropriate temperature and time for solidification. Dry eye patients were divided into 2 groups according to the preparation method of the atelocollagen punctal plug. In the conventional implantation group, atelocollagen gel was kept at room temperature for 15 minutes before implantation (27 eyes of 14 patients). In the preheating group, atelocollagen was warmed at 41 C for 8 minutes before implantation (23 eyes of 13 dry eye patients). Strip meniscometry, vital stainings, tear film break-up time (BUT), and symptom scores were evaluated before and 1 month after plug implantation.
Results
In vitro experiments revealed that heating at 41 C for 8 minutes was sufficient to solidify the gel. The mean fluorescein score in the conventional implantation group significantly improved after treatment (before, 3.5 ± 2.3 points; after, 2.5 ± 0.9 points, P < .05). In the preheating group, the mean fluorescein score (before, 3.7 ± 1.7 points; after, 1.5 ± 1.2 points), strip meniscometry (before, 0.6 ± 0.7 mm; after, 1.1 ± 0.3 mm), BUT (before, 3.2 ± 0.7 seconds; after, 4.8 ± 1.0 seconds), and visual analog scale scores (before, 6.6 ± 1.5 points; after, 4.1 ± 0.9 points) significantly improved after treatment ( P < .05).
Conclusion
The thermosensitive atelocollagen punctal plug was effective for dry eye treatment. The preheating method was found to be useful to strengthen the efficacy of the thermosensitive atelocollagen punctal plug.
Punctal plug insertion has already been reported to be an effective treatment for aqueous tear-deficient dry eye diseases, such as Stevens-Johnson syndrome, contact lens–related dry eyes, and neurogenic dry eyes occurring after laser in situ keratomileusis (LASIK) and photorefractive keratectomy. In 1961, Foulds reported the first punctal plug treatment with gelatin-type punctal plugs. In terms of materials, current punctal plugs are categorized as absorbable and nonabsorbable. Absorbable plugs are mainly used for evaluating the effect with nonabsorbable plugs or treatment of temporary dry eye disease such as post-LASIK dry eyes. The Freeman-style plug is among the most popular nonabsorbable punctal plug design. This plug consists of a cylindrical neck; a wider base that sits at the angle where the vertical and horizontal segments of the canaliculus meet, anchoring it in position; and a wider disc-shaped head or flange that sits on the surface of the punctal opening. The Freeman-style punctal plug is available in various sizes and has been reported to fit most cases of dry eyes. It has been reported to have high stability and safety, with some inherent problems consisting of granulation formation, irritation of cornea and conjunctiva, epithelial laceration, and frequent extrusion. Surgical punctal occlusion by cautery or laser is another option for dry eyes not suitable for punctal plug treatment. However, such treatment options also possess several problems, such as deformation of the punctum, recanalization, and symblepharon formation.
The collagen punctal plug is one of the absorbable plugs and is mainly used for temporary dry eye disease such as postsurgical dry eye or seasonal worsening of dry eye disease. A Cochrane database review concluded that temporary collagen plugs appear similarly effective to silicone plugs on a short-term basis.
Recently, a new generation of thermosensitive atelocollagen punctum plug (Keeptear; Koken Bioscience Institutes, Tokyo, Japan) has been developed and is being widely used in Japan. Briefly, Keeptear is categorized as an absorbable collagen plug and possesses unique characteristics. Keeptear is available in a syringe. Keeptear is made of thermosensitive atelocollagen, which is liquid at room temperature but becomes a soft gel at body temperature. After insertion, as the Keeptear equilibrates to the body temperature, the material softens and fits the patient’s punctum.
According to the manufacturer’s suggestions, Keeptear should be kept at room temperature for 15 minutes after being taken out of the refrigerator, after which it is then injected into the patient’s canaliculus from the punctum. We hypothesized that preheating atelocollagen gel could enhance the treatment effect, and thus we designed this study.
In this study, we evaluated the efficacy of a new punctal plug (Keeptear) insertion method in patients with dry eye disease, comparing the preparation method with conventional methodology.
Methods
The protocol of this prospective randomized clinical study and informed consent were approved by the Institutional Review Board of the Keio University School of Medicine and the study was registered at UMIN-CTR ( http://www.umin.ac.jp/ctr/index.htm ) (UMIN000011574). The study procedures conformed to the ethical principles for research involving human subjects as outlined in the Declaration of Helsinki. Informed consents for both the treatment and participation in the research were obtained from all subjects after explanation of the nature and possible consequences of taking part in the study.
In Vitro Experiments
Keeptear punctal plugs ( Figure 1 , Top left) are made from bovine dermal tissue and prepared with 0.2% concentration by a manufacturing company for clinical use.
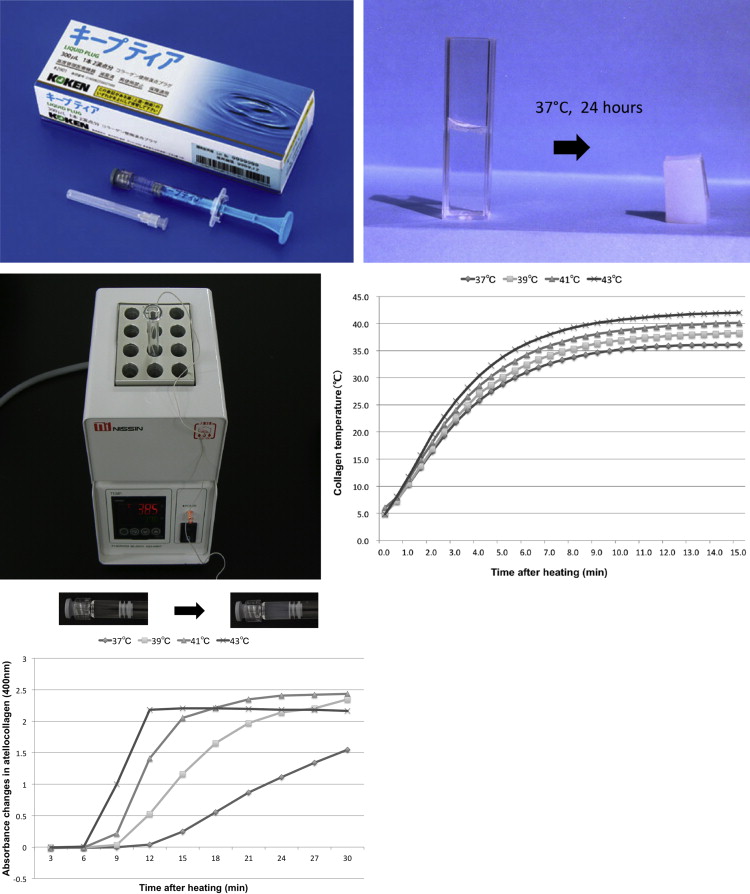
To evaluate and understand the gel formation process of the Keeptear punctal plug, in vitro experiments were designed. The Keeptear atelocollagen punctal plug becomes a soft gel from liquid at 37 C ( Figure 1 , Top right). Initially, to determine the shortest time in which Keeptear reaches the gel form at 37 C, Keeptear was warmed using a thermoblock, which can adjust the temperature ( Figure 1 , Middle left). The timewise changes of collagen temperature were recorded using a thermometer (UV-1200; Shimadzu, Tokyo, Japan). In the in vitro experiments, the thermoblock was warmed to 37 C, 39 C, 41 C, and 43 C. To clarify when the Keeptear started to attain the soft gel form, spectrometry (digital multimeter PC5000a; Sanwa Electric Instrument Inc., Tokyo, Japan) was performed, and absorbance at 400 nm was measured after warming Keeptear at different temperatures.
Clinical Study
Subjects
Keeptear plugs were inserted in a total of 50 eyes of 27 dry eye patients (Sjögren syndrome: 12 patients, non–Sjögren syndrome: 15 patients). Before punctal plug insertion, irrigation of the canaliculus was performed for all patients, and it was confirmed that the tear drainage system was intact. Two preparation methods of Keeptear punctal plugs were randomly assigned to patients. In the conventional implantation group, atelocollagen gel was kept at room temperature for 15 minutes before implantation (27 eyes of 14 patients). In the preheating group, immediately after taking the atelocollagen punctal plug from the refrigerator, it was warmed at 41 C for 8 minutes before implantation (23 eyes of 13 dry eye patients). After plug insertion, patients were asked to use only preservative-free artificial tear eye drops (Softsantear; Santen Pharmaceutical Co Ltd, Osaka, Japan) 6 times a day. Tear functions and ocular surface examinations were performed before and 1 month after treatment. To minimize the effect of each examination on the following examinations, tear volume measurement using strip meniscometry was performed initially. Ten minutes later, tear film break-up time measurements and then vital stainings were performed. A single clinician (T.K.) performed injections of Keeptear punctal plugs and all examinations including tear functions and ocular surface vital stainings. Patient demographics and tear functions/ocular surface abnormalities before thermosensitive atelocollagen punctal plug treatment were shown in Table .
| Conventional Method | Preheating Method | |
|---|---|---|
| Patients (eyes) | 14 (27) | 13 (23) |
| Sex | Female:12, Male: 2 | Female:10, Male:3 |
| Age (y), mean ± SD | 61.3 ± 17.2 | 62.4 ± 14.5 |
| Pretreatment tear functions and ocular surface abnormalities | ||
| Schirmer I test (mm) | 5.4 ± 2.0 | 5.1 ± 2.7 |
| Tear film break-up time (seconds) | 3.3 ± 1.1 | 3.4 ± 0.8 |
| Fluorescein score (points) | 3.6 ± 2.4 | 3.8 ± 1.7 |
| Rose bengal score (points) | 2.2 ± 1.9 | 2.0 ± 1.4 |
Punctal plug procedure
A 26 G blunt-tip needle was used for insertion. A total of 150 μL of Keeptear was injected into each upper and lower punctum. If backflow of collagen was observed, injection was stopped. Immediately following insertion, a warm compress (hot eye mask, Kao Corporation, Tokyo, Japan) was placed onto the patients’ eyelids for 10 minutes. Plugs were inserted in both superior and inferior lacrimal puncta in all patients.
Strip meniscometry testings
The tip of the meniscometry strip was inserted for 5 seconds into the lateral lower tear meniscus without touching the ocular surface. The duration of the test was measured strictly by a stopwatch chronometer at each testing. The length of the stained tear column in the central membrane ditch was regarded as the strip meniscometry value in that eye in millimeters. The SM testing has been reported to be useful in the evaluation of tear meniscus volume, as reported previously.
Tear function tests
The standard tear film break-up time (BUT) measurement was performed after instillation of a 2-μL volume of a 0.5% fluorescein dye in the conjunctival sac with a micropipette. A cobalt blue filter was used to measure the BUT. The patients were then instructed to blink several times for a few seconds to ensure adequate mixing of the dye. The interval between the last complete blink and the appearance of the first corneal black spot in the stained tear film was measured 3 times and the mean value of the measurements was calculated.
Vital stainings
Fluorescein stain scoring of the ocular surface was performed. The fluorescein staining scores of the ocular surface ranged from 0-9 points. In fluorescein and rose bengal staining, the ocular surface was divided into 3 parts: temporal conjunctiva, cornea, and nasal conjunctiva. Each zone had a staining score ranging from 0-3 points, with the minimum and maximum total staining scores ranging from 0-9 points.
Evaluation of dry eye symptoms
Symptoms of “dryness” were evaluated with visual analog scale (VAS) scores. Participants indicated scores on the VAS sheets before and 1 month after treatment. Lower scores on the VAS referred to a less severe degree of symptoms, whereas higher VAS scores indicated severe symptoms in this study (minimum: 0 point, maximum: 10 points).
Dry eye diagnostic criteria
The diagnosis of dry eye disease was based on the diagnostic criteria of the Dry Eye Research Group in Japan. In brief, patients with (1) dry eye–related symptoms; (2) positive staining with fluorescein or rose bengal dyes; and (3) Schirmer I test results of less than 5 mm, or tear film BUT values of less than 5 seconds were diagnosed as having dry eyes. A fluorescein staining score above 3 points and a rose bengal staining score above 3 points was considered abnormal. Dry eye cases were categorized as Sjögren syndrome (SS) and non-SS on the basis of the criteria proposed by Fox and associates.
Statistical analysis
For statistical analyses, paired t test was used for comparisons of tear functions and ocular surface tests before and after punctal plug insertion. A P value less than .05 was considered statistically significant. Data were processed using the IBM SPSS Statistics software (IBM, Armonk, New York, USA) for Macintosh OS X (Apple, Cupertino, California, USA).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


