Chapter 9
EVALUATION

GENERAL EVALUATION
Prior to taking a history and performing an examination focused on the eye, the ophthalmologist must “take a step back” and assess the whole patient. In many cases with multiple injuries or polytrauma, an ER trauma team initiates the treatment, first focusing on any life-threatening injury (see Chapter 10). In this scenario, the ophthalmologist is usually called for consultation after the patient is stabilized and may have no immediate role in the triage process. Typically, however, the eye trauma patient presents directly to the ophthalmologist. In such cases, it is important to keep in mind that the patient may have sustained nonglobe injuries (e.g., occult stab/gunshot wound to the chest, fracture, closed head trauma) that may be life threatening and must be addressed first.
PEARL… Always be suspicious of an undiagnosed injury to other organ systems.
Initial Systemic Triage
When accepting an ocular trauma patient directly or from another facility, the general status of the patient should be ascertained so that the appropriate triage pathway can be chosen (i.e., transfer to a general trauma ER or to an eye hospital).
• Record vital signs along with an assessment of the mental status.
• Quickly examine the patient for evidence of obvious bone or severe soft-tissue injury before concentrating on the eye examination.
• Transfer the ocular trauma patient immediately to a general ER or trauma facility if during the rapid primary assessment any of the following signs are present:
 unstable vital signs;
unstable vital signs;
 impaired mental status; or
impaired mental status; or
 serious nonocular injuries.
serious nonocular injuries.
Once it is determined that the patient is stable and the eye injury can be addressed, a more general medical/surgical history should be taken, documenting:
• all medical conditions;
• current medications;
• drug allergies;
• prior surgeries;
• history of any complications during anesthesia;
• tetanus immunization status (toxoid is recommended in all cases of open globe injury when immunization is not up to date or when an adequate vaccination history cannot be obtained; also see Chapter 8 and the Appendix); and
• the time when the patient last ate or drank (see Chapter 8).
Special Considerations for the Elderly Patient Falls resulting in eye/orbital trauma may also cause fractures of the hip, long bones, and skull with or without subdural/intracerebral hemorrhage. Any underlying or associated conditions and the cause of the fall should be ascertained as:
• falls associated with loss of consciousness or syncope may indicate underlying cardiovascular disease (e.g., arrhythmia) or hypotension, requiring further investigation;
• significant, even potentially life-threatening, internal bleeding may occur despite mild trauma if the patient is receiving anticoagulation therapy;
• elderly patients may have underlying dementia, making it difficult to obtain a clear history of the events leading to the injury. In such cases, it can be helpful to interview family members and/or care-givers (see Chapter 10).
The examiner must always be alert to the possibility of abuse or neglect. Understanding the patient’s home environment/living arrangement is critical for discharge planning in the aftermath of a serious eye injury. In many instances, family members and/or social services need to be engaged to effect a smooth transition from hospital to home/assisted living.
Special Considerations in Children (Also see Chapters 8 and 30)
Eliciting an accurate history can be difficult due to:
• unwillingness of the child to admit engaging in forbidden behavior (e.g., playing with a BB gun or fireworks);
• reluctance on the caregiver’s part to volunteer basic information about the circumstances and mechanism of the injury. This should alert the ophthalmologist to the possibility of child abuse, poor supervision, neglect, or significant occult injury. A complete ophthalmic examination with meticulous documentation should be performed. If abuse is suspected, a social worker should be contacted so that the appropriate protective service agencies can be engaged.
PEARL… Inability to perform an adequate pediatric examination in the office should prompt the scheduling of a formal examination under sedation or general anesthesia.
OPHTHALMOLOGIC EVALUATIONa
History
Although a thorough ophthalmic examination usually reveals the nature of the ocular injury, a focused history may rapidly direct the examiner to the critical findings as well as provide important information for guiding initial management and assessing prognosis. A precise, well-documented history in the medical record is also useful for future legal proceedings (see Chapter 7).
It is best to allow the patient to tell his “story.” It is important to resist the temptation to interrupt and interrogate the patient immediately in a busy ER setting, although periodic redirection is commonly necessary. The history should include the following.
The context and events leading up to the injury
• Location; and appropriate associated factors such as the use or misuse of safety glasses; seat belt use; air bag deployment and whether the injury has indeed been caused by it.b
A detailed description of the mechanism of the injury
• Blunt objects may cause rupture or contusion, as opposed to sharp objects that lead to laceration (see Chapter 1) with a usually more favorable prognosis1 (see Chapter 3).
• It is a critical part of the Standardized Ocular Trauma Classification System2,3 (see Chapter 2).
The exact time of the injury
• Knowing the time from injury to presentation is mandatory in planning the treatment strategy (see Chapter 8). Unlike fresh, open wounds, a quiet eye with a 1-week-old, self-sealing corneal laceration may be managed more conservatively.
The place of the injury
• Open globe injuries occurring in a rural setting have a much higher risk of infection than comparable injuries in nonrural settings.4
The composition of the IOFB (see Chapter 24) and the identity of any chemical agent (see Chapter 11)
Prior ocular history
• Ophthalmic surgery and/or trauma (risk factors for rupture, see Chapter 27).
• The preinjury vision and the visual potential of the fellow eye.
• Any ocular medications.
Key aspects of external inspection include the following.
• Inspect the head, scalp, face, periorbital tissues, and eyelids under bright illumination. Check for lacerations, ecchymoses, obvious protruding foreign bodies, lid and periorbital edema, ptosis, and the presence/absence of enophthalmos or exophthalmos by Hertel prism measurements.
• Inspect the globes without the aid of magnification for evidence of:
 protruding foreign bodies (see Chapter 24);
protruding foreign bodies (see Chapter 24);
 gross prolapse of intraocular contents; and
gross prolapse of intraocular contents; and
 occult open globe injury in case of appropriate history (e.g., fistfight; hammering; previous eye surgery/trauma), reduced vision, small lid wound, irregular (peaked) pupil, and hemorrhagic chemosis (Fig. 9–1);
occult open globe injury in case of appropriate history (e.g., fistfight; hammering; previous eye surgery/trauma), reduced vision, small lid wound, irregular (peaked) pupil, and hemorrhagic chemosis (Fig. 9–1);
 pronounced unilateral exophthalmos (may suggest a traumatic carotid-cavernous fistula).
pronounced unilateral exophthalmos (may suggest a traumatic carotid-cavernous fistula).
• Palpate the scalp, face and periorbital soft tissue for: ° occult subcutaneous foreign bodies and signs
that, even without Hertel measurement asymmetry, strongly suggest the presence of an orbital fracture: ° crepitus;
 step-off deformities; and
step-off deformities; and
 infraorbital hypesthesia.
infraorbital hypesthesia.

FIGURE 9–1 A penlight or flashlight can be used to assess the eye rapidly. Gentle traction with a lid speculum exposes the globe, revealing a full-thickness injury. The IOFB is not removed until the patient is in the operating room.
PEARL… If lid edema is present, a speculum or retractor may be used to visualize the globe, but extreme care should be taken not to exert pressure on the globe, causing extrusion of ocular contents (see Fig. 9–2 and Chapter 8). In cases of very swollen lids or an uncooperative patient, it is better to forgo speculum/retractor use and proceed directly to an imaging study (see later in this Chapter).
Young childrenc may need to be restrained (see Chapters 8 and 30). If this is impossible or the child feels more secure when in direct contact with the parent, follow the steps given below.
1. An assistant and parent sit at the same level facing each other.
2. The child is positioned supine with legs straddling the parent’s waist.
3. The child’s head is placed on the assistant’s lap.
4. The parent holds the child’s hands and legs.
5. The assistant holds the child’s head still while the physician performs the examination.

FIGURE 9–2 Shortly after slit-lamp examination, this patient developed a hemorrhagic choroidal detachment with extrusion of intraocular contents.
| Explain procedures to the patient in advance, especially children. |
| Reassure the patient that you can help him/her. |
| Never patch both eyes unless both eyes are injured. Covering both eyes only heightens concern about impending blindness. |
| Place the patient in a calm, quiet setting and be mindful of the patient’s privacy/modesty. |
| Be realistic but not overly pessimistic about potential outcomes. The patient should understand the severity of the eye injury, but this message should be delivered with com-passion as well as candor. In all but the most hopeless of cases, the examiner should impart a sense of hope and optimism in discussions regarding prognosis. |
* See also Chapters 5, 7, and 8.
If an adequate examination is not possible without the risk of extrusion of ocular contents, the examination should be carried out under sedation. A qualified anesthesiologist or critical care specialist should administer anesthesia in a monitored setting, with access to advanced life-support medication and equipment (see Chapter 8).
Anxiety is commonly present and should be addressed (see Table 9–1).
Visual Function Testing
Central Vision
The presenting visual acuity is a crucial prognostic indicator (see Chapter 3).
Visual acuity is measured in each eye separately,using an occluder or eye patch. Particularly in younger patients, care should be taken to ensure that the patient does not “cheat” or inadvertently use the fellow eye.
Whenever possible, a standardized chart (e.g., Snellen, ETDRS) should be used.
• Illiterate charts (e.g., E, Landholt C) should be used for patients unable to read.
• For preliterate children use Allen cards, HOTV letters, or the E game.
• In infants, fixation and smooth pursuit can be assessed by using colorful targets, toys, or a hand light.
If feasible, the patient’s best correction should be used to record the visual acuity.
• Because it is rarely possible/practical to perform a formal refraction in an ER setting, the pinhole acuity can be used as a substitute.
For patients with severe ocular injuries or who are immobilized on a stretcher:
• a near card is utilized;
• if vision is too poor to be measured with standard charts, a gross assessment of the visual acuity should be obtained (e.g., counting fingers at a specific distance; hand motions; light perception with projection; light perception without projection; bare light perception; and NLP);
• light perception must be tested using a strong light source (e.g., IBO or slit lamp, never a candle).
Optic Nerve/Retinal Testing
• The presence/absence of an APD is a crucial indicator of gross visual function.d The test is performed utilizing a bright light source (e.g., the IBO at its highest setting). The light source is alternately directed at each eye in a swinging or back-and-forth fashion. The eye with the relative afferent deficit paradoxically dilates when exposed to the light source because the consensual pupillary response in one eye always mirrors the direct pupillary response in the fellow eye.
PEARL… The absence or presence of an APD can be assessed even if the iris is injured. Rather than examining the direct pupillary response in each eye with each swing, only the reactive, intact pupil is observed. If an APD is present, the pupil of the fellow eye dilates when the light is shone into the injured eye.
The presence of an APD may indicate optic nerve damage or significant retinal damage and has prognostic significance (see Chapter 3).
PEARL… APD caused by media opacity (e.g., hyphema, dense cataract) is very rare.
• The patient’s subjective perception of brightness when confronted with a light source is used to estimate optic nerve function. The IBO or a hand-held transilluminator is directed at the normal eye and the patient is instructed that this level of brightness represents a value of 100%. The light is then redirected into the injured eye, and the patient is asked to compare the levels of brightness. If the level is reduced, the patient is asked to quantify the relative amount of brightness (e.g., 10%, 50%, 80%).
• Rapid assessment of the patient’s peripheral visual field can provide additional information about the eye’s overall visual function. Field abnormalities may indicate optic nerve damage or retinal injury.
 Gross visual field testing can be performed quickly and effectively by finger confrontation.e
Gross visual field testing can be performed quickly and effectively by finger confrontation.e
 Formal kinetic/static perimetry is not performed in the acute ER setting, even though it is a sensitive means of following TON over time.
Formal kinetic/static perimetry is not performed in the acute ER setting, even though it is a sensitive means of following TON over time.
• Color vision testing may also detect optic nerve deficits. Color plates (e.g., Hardy-Rand-Rittler, Ishihara) can be used in cases in which the vision is 20/400 or better. If color plates are not available, a red object can be used to test for red desaturation:when optic nerve damage is present, the red object is perceived as grayish or “washed out” when compared with the color seen by the normal fellow eye.
Motility
• The assessment of ocular motility is most relevant in cases of known or suspected cranial nerve and/or orbital injury.
• Significant periorbital edema, hemorrhage, or lack of patient cooperation often prohibits formal motility testing.
• Forced duction testing may be useful to rule out muscle entrapment if orbital wall fracture is suspected (see Chapter 36). The test is contraindicated in case of (potential) open globe injury.
Slit Lamp
PEARL… Although slit-lamp biomicroscopy and IBO are the preferred methods, a rapid assessment can often be made with the use of a simple pen- or flashlight.
Conjunctiva
Foreign bodies and/or chemical precipitates may be sequestered in redundant folds of chemotic conjunctiva or hidden in the fornices (see also Chapters 11 and 13).
• The fornix should be carefully probed and the lids everted using topical anesthetic (see Chapter 13).
• Hemorrhagic chemosis raises the possibility of orbital fracture and/or open globe trauma.
• Lacerations of the conjunctiva may not be obvious initially but can be detected with gentle manipulation of the conjunctiva using a cotton-tip swab. Once a conjunctival laceration is identified, attention should be focused on ruling out an underlying scleral wound or a subconjunctival foreign body.
Cornea
The examination begins on the surface, then proceeds more deeply (see also Chapter 14).
• Epithelial defects may require topical fluorescein staining.
• Fresh woundsf must be carefully evaluated to determine whether they are full thickness. A full-thickness wound leaks aqueous (although gentle pressure may have to be applied), which can be highlighted by using 2% fluorescein. Under blue light, egress of aqueous fluid dilutes the topical fluorescein dye, forming a green stream in the middle of a more stagnant pool of bright yellow dye (“Seidel positive”; see also Chapters 14 and 19).
• Superficial foreign bodies. If the foreign body spans the cornea into the AC, it is an open globe injury and the object is best removed in the operating room; see Fig. 9–3).
• Abrasions, opacities, and ulcerations. The examiner should always assume an open globe injury until proved otherwise.
Sclera
The conjunctiva may remain intact overlying a full-thickness wound or the two wounds may be distant from each other (see Chapter 13). Hemorrhage in or under the conjunctiva may also hide the scleral lesion. If the presence of a scleral wound cannot be ruled out under the slit lamp, exploratory surgery may have to performed.
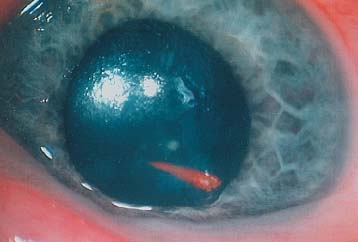
FIGURE 9–3 A transcorneal pricker extends into the AC. Although the external end could be grasped at the slit lamp, it was removed and the wound sutured in the operating room.
Anterior Chamber
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


