Purpose
To provide a diagnostic approach for the evaluation of patients with exaggerated, prolonged, or delayed postoperative intraocular inflammation.
Design
Perspective.
Methods
Selected articles on normal and abnormal postoperative intraocular inflammation were reviewed and interpreted in the context of the authors’ clinical and research experience.
Results
In addition to infectious endophthalmitis, a number of noninfectious conditions characterized by exaggerated, prolonged, or delayed postoperative inflammation have been described. Heuristically, increased postsurgical inflammation may be categorized by time from surgery to first recognition using the following general guidelines: as immediate and occurring within 2 days after surgery; as early and occurring after 2 days, but within the first 2 weeks, after surgery; and as delayed and occurring more than 2 weeks after surgery.
Conclusions
Although infectious endophthalmitis always must be excluded as a cause of increased postoperative intraocular inflammation, potential noninfectious causes also exist. We review both infectious and noninfectious causes of increased postoperative inflammation and provide a diagnostic framework for evaluating such patients.
Demand for ophthalmic surgery is high and is increasing worldwide. It has been estimated, for example, that in excess of 10 million cataract surgeries are performed globally each year. This number is projected to increase dramatically over the coming decades, related both to population growth and aging. In the United States alone, the number of cataract procedures is expected to increase by 50% by 2020, the largest projected increase in any single surgical procedure, regardless of specialty. Similar increases are expected in the number of other ophthalmic procedures, including glaucoma and vitreoretinal surgeries.
Mild postoperative inflammation accompanies all intraocular surgeries. Whereas the severity of the inflammatory response, which has been studied most extensively in cataract surgery, may vary with the type of procedure performed, inflammation after most uncomplicated intraocular surgeries tends to resolve within a matter of weeks, with or without treatment. Hence, the occurrence of exaggerated, prolonged, or delayed postsurgical inflammation can be a cause for considerable concern. The purpose of this perspective is to provide a diagnostic approach for evaluating patients with abnormal postoperative inflammation.
Normal Postoperative Inflammation
Surgical manipulation induces a breakdown of the blood-aqueous barrier, which generally reaches a nadir within the first few postoperative days and then progressively recovers over 2 to 3 weeks after surgery. Detailed information regarding what constitutes normal postoperative inflammation can be gleaned by studying the placebo groups of randomized controlled clinical trials designed to evaluate the efficacy of topical anti-inflammatory medications used to treat routine postsurgical inflammation, including both nonsteroidal anti-inflammatory drugs and corticosteroids. In a recent trial comparing 0.09% bromfenac ophthalmic solution (Xibrom; ISTA Pharmaceuticals, Inc, Irvine, California, USA) versus placebo, for example, the placebo group had a mean anterior chamber cell grade of 2+ on postoperative day 1 and of 1+ on postoperative day 15 ( Figure 1 ). Comparable trends were seen for postoperative flare and pain relief. Similarly, a recent trial of 0.05% difluprednate ophthalmic emulsion (Durezol; Alcon, Inc, Fort Worth, Texas, USA) versus placebo demonstrated a comparable time course for improvement of postoperative inflammation and symptoms. Although similar placebo-controlled studies are not available for glaucoma or vitreoretinal surgery, it is generally assumed that comparable trends would be observed after uncomplicated procedures.
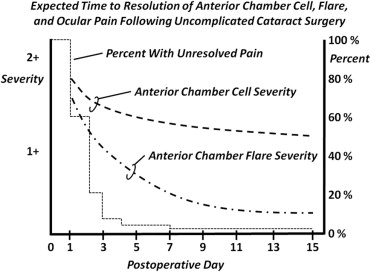
Based on these findings, it is estimated that a grade of 2+ anterior chamber cell on postoperative day 1 and of 1+ cell on postoperative day 14 should be considered within normal limits after uncomplicated anterior segment surgery. Substantial pain is unusual beyond postoperative day 2 or 3 and should raise suspicion of infection. Potential noninfectious causes of excessive pain or discomfort beyond this period include acutely increased intraocular pressure, exposed suture material, or the presence of an epithelial defect.
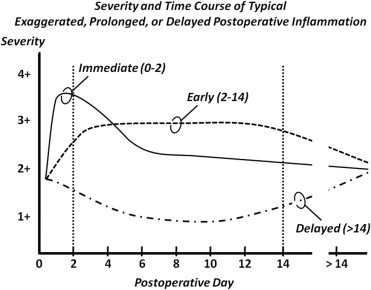
Given the many possible causes for abnormal postoperative inflammation, we have found it to be helpful heuristically to broadly categorize exaggerated, prolonged, or delayed postsurgical inflammation by time from surgery to first recognition as: (1) immediate and occurring within 2 days after surgery; (2) early and occurring after 2 days, but within the first 2 weeks, after surgery; or (3) delayed and occurring more than 2 weeks after surgery ( Figure 2 ). It is important to remember, however, that time to presentation or recognition for any of the conditions summarized below may vary from patient to patient and that the specific time designations should be viewed as guidelines.
Immediate Presentation
Notable causes of markedly increased inflammation to consider during the first 2 days after surgery include endophthalmitis, toxic anterior segment syndrome, and complicated surgery.
Endophthalmitis
Endophthalmitis remains the most dreaded and immediately sight-threatening complication after intraocular surgery and always should be first on the list of causes for exaggerated postoperative inflammation. The presence of pain, chemosis, eyelid edema, and diffusely distributed keratic precipitates should increase the suspicion for an infectious cause. Reported incidence rates of endophthalmitis after cataract extraction have ranged from 0.05% to 0.68%, with some having suggested a higher incidence after the increased use of clear corneal incisions.
Theoretically, any organism can cause endophthalmitis presenting in the first 2 postoperative days if the inoculum is large enough. For example, although fungi generally are considered to cause more delayed or chronic endophthalmitis, a retrospective series of 27 cases of fungal endophthalmitis after cataract surgery in India reported 3 cases that occurred within 48 hours of surgery. In these particular cases, the authors noted that an early presentation was suggestive of a large inoculum.
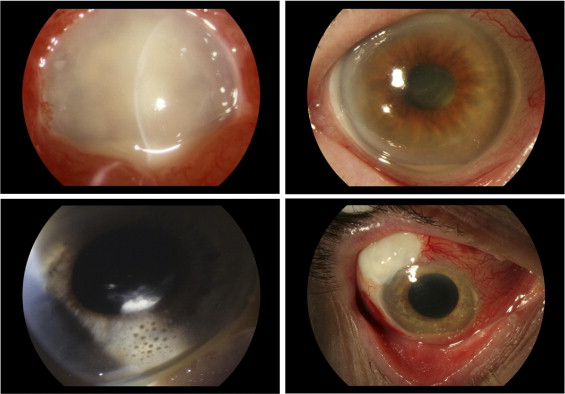
Commonly, however, endophthalmitis that manifests during the first 2 postoperative days results from infection by a more virulent organism, such as Pseudomonas ( Figure 3 ) or Streptococcus. In the Endophthalmitis Vitrectomy Study (EVS), for example, approximately one third of cases sought treatment within the first 2 postoperative days. These eyes were more likely to harbor infections with Gram-negative organisms or Gram-positive organisms other than coagulase-negative cocci than eyes first treated 3 days or more after surgery. In a retrospective analysis of all patients with postoperative endophthalmitis seen at Aravind Eye Hospital in Madurai, South India, from 1997 to 2006, Pseudomonas comprised 43% of what the authors termed the fulminant type of endophthalmitis, defined as occurring within 4 days of surgery, whereas Pseudomonas accounted for less than 7% of endophthalmitis occurring after this period. Similarly, of 9 cases of Pseudomonas endophthalmitis after cataract extraction diagnosed at Bascom Palmer Eye Institute in Miami, Florida, from 1987 to 2001, the median time to presentation was 4 days, with 3 cases seeking treatment within the first 2 days. Visual prognosis in patients with Pseudomonas or Streptococcus endophthalmitis tends to be poor. In the EVS, for example, 3 of 4 patients with Pseudomona s endophthalmitis had a visual acuity outcome worse than 5/200. In a recent series analyzing postcataract endophthalmitis treated at a single institution in The Netherlands, all 21 cases with culture-proven Streptococcus pneumoniae or beta-hemolytic Streptococcus sought treatment in the first 3 postoperative days, and only 1 of these achieved a visual acuity outcome better than 20/40.
Toxic Anterior Segment Syndrome
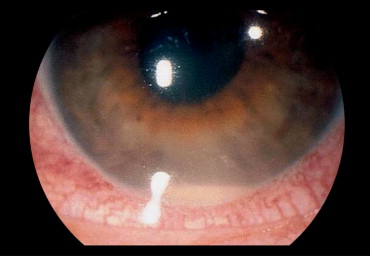
Toxic anterior segment syndrome is a noninfectious cause of inflammation typically manifested during the first 24 hours after anterior segment surgery. It often is attributed to impurities in surgical fluids or instruments, and also may be caused by foreign material entering a clear corneal incision during or after surgery. Common findings include fibrin formation and diffuse corneal edema related to damage to the corneal endothelium. The intraocular pressure tends to be low initially because of ciliary body shutdown, but later may spike as damage to the trabecular meshwork limits aqueous outflow. Toxic anterior segment syndrome often is distinguished from endophthalmitis by less prominent redness and pain, and by what tends to be a less severe anterior chamber reaction and little or no vitreous inflammation—although more severe anterior chamber inflammation can occur ( Figure 4 ). Gram stain and cultures show negative results, and patients frequently respond well to topical corticosteroids alone. Although most often recognized within 1 or 2 days of surgery, toxic anterior segment syndrome related to polishing materials used on intraocular lenses has been reported to occur up to 21 days after surgery. Long-term recovery depends on the degree of damage to the corneal endothelium, trabecular meshwork, and ciliary body.
Complicated Surgery
A greater than expected degree of postoperative inflammation may be associated with more involved procedures, longer operative times, intraoperative complications, prior surgery, and younger patient age. A study using fluorophotometry to measure anterior chamber inflammation in rabbit eyes, for example, demonstrated greater inflammation with a larger incision, a larger capsulorrhexis, and a sulcus versus in-the-bag intraocular lens placement. Thus, deviations from normal surgical routine may alter the expected course of postoperative inflammation and symptoms. Although the contribution of surgical complications to the level of postoperative inflammation generally is obvious and well understood by the operating surgeon, such complications and associated surgical manipulation also may increase the risk of subsequent infection. Care still should be taken, therefore, to exclude the possibility of postoperative endophthalmitis, particularly when the inflammation is persistent or disproportionate to the degree of difficulty encountered during surgery.
Immediate Presentation
Notable causes of markedly increased inflammation to consider during the first 2 days after surgery include endophthalmitis, toxic anterior segment syndrome, and complicated surgery.
Endophthalmitis
Endophthalmitis remains the most dreaded and immediately sight-threatening complication after intraocular surgery and always should be first on the list of causes for exaggerated postoperative inflammation. The presence of pain, chemosis, eyelid edema, and diffusely distributed keratic precipitates should increase the suspicion for an infectious cause. Reported incidence rates of endophthalmitis after cataract extraction have ranged from 0.05% to 0.68%, with some having suggested a higher incidence after the increased use of clear corneal incisions.
Theoretically, any organism can cause endophthalmitis presenting in the first 2 postoperative days if the inoculum is large enough. For example, although fungi generally are considered to cause more delayed or chronic endophthalmitis, a retrospective series of 27 cases of fungal endophthalmitis after cataract surgery in India reported 3 cases that occurred within 48 hours of surgery. In these particular cases, the authors noted that an early presentation was suggestive of a large inoculum.
Commonly, however, endophthalmitis that manifests during the first 2 postoperative days results from infection by a more virulent organism, such as Pseudomonas ( Figure 3 ) or Streptococcus. In the Endophthalmitis Vitrectomy Study (EVS), for example, approximately one third of cases sought treatment within the first 2 postoperative days. These eyes were more likely to harbor infections with Gram-negative organisms or Gram-positive organisms other than coagulase-negative cocci than eyes first treated 3 days or more after surgery. In a retrospective analysis of all patients with postoperative endophthalmitis seen at Aravind Eye Hospital in Madurai, South India, from 1997 to 2006, Pseudomonas comprised 43% of what the authors termed the fulminant type of endophthalmitis, defined as occurring within 4 days of surgery, whereas Pseudomonas accounted for less than 7% of endophthalmitis occurring after this period. Similarly, of 9 cases of Pseudomonas endophthalmitis after cataract extraction diagnosed at Bascom Palmer Eye Institute in Miami, Florida, from 1987 to 2001, the median time to presentation was 4 days, with 3 cases seeking treatment within the first 2 days. Visual prognosis in patients with Pseudomonas or Streptococcus endophthalmitis tends to be poor. In the EVS, for example, 3 of 4 patients with Pseudomona s endophthalmitis had a visual acuity outcome worse than 5/200. In a recent series analyzing postcataract endophthalmitis treated at a single institution in The Netherlands, all 21 cases with culture-proven Streptococcus pneumoniae or beta-hemolytic Streptococcus sought treatment in the first 3 postoperative days, and only 1 of these achieved a visual acuity outcome better than 20/40.
Toxic Anterior Segment Syndrome
Toxic anterior segment syndrome is a noninfectious cause of inflammation typically manifested during the first 24 hours after anterior segment surgery. It often is attributed to impurities in surgical fluids or instruments, and also may be caused by foreign material entering a clear corneal incision during or after surgery. Common findings include fibrin formation and diffuse corneal edema related to damage to the corneal endothelium. The intraocular pressure tends to be low initially because of ciliary body shutdown, but later may spike as damage to the trabecular meshwork limits aqueous outflow. Toxic anterior segment syndrome often is distinguished from endophthalmitis by less prominent redness and pain, and by what tends to be a less severe anterior chamber reaction and little or no vitreous inflammation—although more severe anterior chamber inflammation can occur ( Figure 4 ). Gram stain and cultures show negative results, and patients frequently respond well to topical corticosteroids alone. Although most often recognized within 1 or 2 days of surgery, toxic anterior segment syndrome related to polishing materials used on intraocular lenses has been reported to occur up to 21 days after surgery. Long-term recovery depends on the degree of damage to the corneal endothelium, trabecular meshwork, and ciliary body.
Complicated Surgery
A greater than expected degree of postoperative inflammation may be associated with more involved procedures, longer operative times, intraoperative complications, prior surgery, and younger patient age. A study using fluorophotometry to measure anterior chamber inflammation in rabbit eyes, for example, demonstrated greater inflammation with a larger incision, a larger capsulorrhexis, and a sulcus versus in-the-bag intraocular lens placement. Thus, deviations from normal surgical routine may alter the expected course of postoperative inflammation and symptoms. Although the contribution of surgical complications to the level of postoperative inflammation generally is obvious and well understood by the operating surgeon, such complications and associated surgical manipulation also may increase the risk of subsequent infection. Care still should be taken, therefore, to exclude the possibility of postoperative endophthalmitis, particularly when the inflammation is persistent or disproportionate to the degree of difficulty encountered during surgery.
Early Presentation
Notable causes of exaggerated postoperative inflammation to consider after 2 days, but within the first 2 weeks, after surgery include endophthalmitis, retained lens fragments, and conditions known to predispose patients to more severe postoperative inflammation, such as preexisting diabetic retinopathy or uveitis.
Endophthalmitis
Although any organism may cause early endophthalmitis, both coagulase-negative Staphylococcus and Staphylococcus aureus should be considered high on the list of causes during the first 2 postoperative weeks ( Figure 3 ). In the EVS, for example, coagulase-negative cocci accounted for more than half of all cases seeking treatment after day 2, with most cases seeking treatment in the first postoperative week. In the large series of endophthalmitis after clear corneal cataract surgery reported by Lalwani and associates, the mean time from surgery to diagnosis for all organisms was 13 days, and coagulase-negative Staphylococcus and S. aureus accounted for 58% and 13% of cases, respectively, seeking treatment during the first postoperative week. Similarly, of 20 cases of postcataract extraction endophthalmitis treated at an eye hospital in Saudi Arabia over a 10-year period, half of all cases seeking treatment the first 2 weeks were the result of these organisms. Although typically less fulminant and severe than either Pseudomonas or Streptococcus endophthalmitis, Staphylococcus infections also can be associated with poor visual outcomes. In a review of 32 cases of culture-proven S. aureus endophthalmitis seen at Bascom Palmer, a visual acuity of 20/400 or better at 3 months of follow-up was achieved in only 59% of eyes infected with methicillin-sensitive S. aureus and 36% of eyes infected with methicillin-resistant S. aureus.
Endophthalmitis after vitreoretinal surgery also typically occurs within the first postoperative week. In a review of all patients with endophthalmitis after pars plana vitrectomy at 1 institution over a 20-year period by Eifrig and associates, the mean time from surgery to diagnosis was 3 days, with a range from 1 to 6 days. Three of the 6 cases were the result of S. aureus , 1 case was the result of Proteus mirabilis , a third bore a coinfection with Staphylococcus epidermidis and Pseudomonas , and the final case was culture negative. A separate study of 18 patients with postvitrectomy endophthalmitis drawn from 8 different clinical centers noted that all cases sought treatment within 8 days of surgery, with an average of 3 days to presentation. Coagulase-negative Staphylococci were present in 9 patients (2 were coinfected with Streptococcus ), and S. aureus was present in an additional 4 patients.
Retained Lens Material
As previously noted, eyes with more complicated surgery tend to have more marked postoperative inflammation. Multiple factors may contribute to the increased inflammation, including capsular rupture, vitreous loss or incarceration in the wound, and intraocular lens capture by the iris, among others. Although technically a complication of surgery, and often clinically obvious ( Figure 5 ), we address retained lens material separately because small amounts of retained cortex or nucleus either may go unrecognized or may not be considered a complication at the time of surgery.



