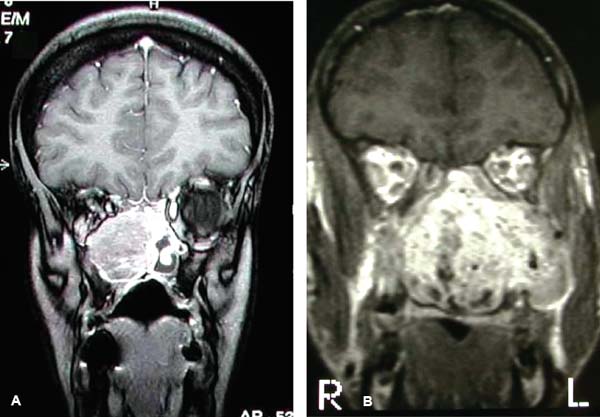
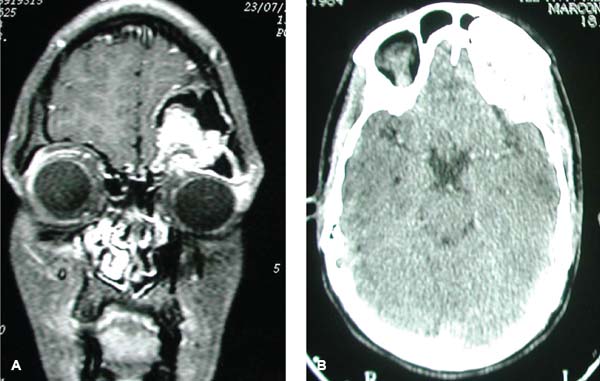
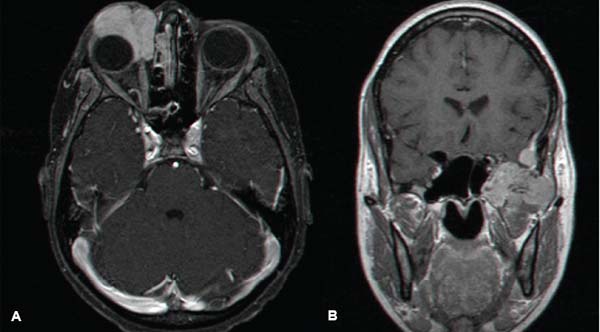
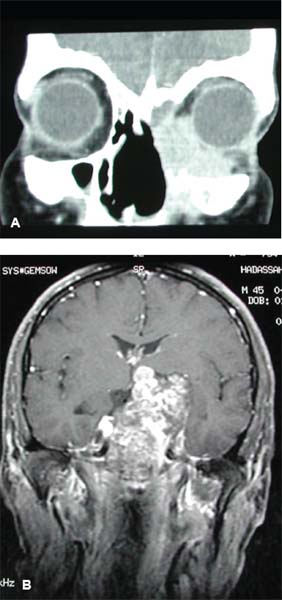
15 Core Messages • Tumors of the nasal cavity and paranasal sinuses account for only 3% of all head and neck tumors, and ethmoid tumors are found in 20 to 30% of all paranasal malignancies. • Primary ethmoid tumors invade via the route of least resistance, which includes the nasal cavity, paranasal sinuses, nasopharynx, lamina papyracea, and cribriform plate. • The most common of malignant neoplasms in this group is squamous cell carcinoma, and the most common benign tumor is inverted papilloma. • Signs and symptoms can often be misleading and initially interpreted as infectious and benign disease. A high degree of suspicion is necessary for any symptom suggestive of a growing tumor in the nasal cavity and sinuses. • The physical examination should always include a fiberoptic endoscopic evaluation of the nose, sinuses, nasopharynx, and oropharynx. Special attention should also be paid to the presence of facial asymmetry, proptosis, serous otitis media, and cranial nerve palsies. • Computed tomography (CT) and magnetic resonance imaging (MRI) are the modalities of choice for staging and follow-up of skull base tumors. The main advantage of CT scans is their superiority in delineating the architecture of the bones, and the main advantage of MRI is its supremacy in delineating among soft-tissue structures. • Tissue diagnosis is crucial for the tailoring of treatment and should always be performed after a proper imaging work-up. Tissue is usually obtained by means of endoscopic biopsy under local anesthesia. • Malignant tumors of the ethmoids and anterior skull base are almost always treated by surgery. Exceptions are lymphomas and small cell carcinomas, which are managed by chemoradiation. • The classical resections of malignant tumors of the anterior skull base and ethmoids are performed via the open craniofacial approach. Recent developments in minimally invasive modalities have led to the popularization of endoscopic surgery for resection of both benign and malignant tumors. • The overall 5-year survival of patients with malignant tumors of the anterior skull base is 50%. Their prognosis depends, above all else, on histology and margin status. • The overall quality of life in the majority of patients after anterior skull base tumor extirpation can be classified as “good,” with significant improvement taking place within 6 months after surgery. Tumors involving the ethmoid sinus and anterior skull base represent a group of varying histologies with distinct clinical implications. The route of spread of tumors originating in the anterior skull base and ethmoid sinuses is determined by the complex anatomy of the craniofacial compartments. Over the last four decades, advancements in imaging modalities, development of minimally invasive techniques, and refinements in surgical and reconstructive methods have enabled an increasing number of patients with skull base neoplasms to undergo curative surgical resections. Benign tumors of the ethmoid complex are usually treated by endoscopic surgery, whereas malignant tumors with anterior skull base invasion are treated by craniofacial resection or endonasal surgery with adjuvant radiation therapy. This chapter reviews the evaluation and management of the ethmoid complex and anterior skull base neoplasms. The surgical results and quality of life (QOL) of these patients are also discussed. Tumors of the nasal cavity and paranasal sinuses account for only 3% of all head and neck tumors, and ethmoid tumors are found in 20 to 30% of all paranasal malignancies. Malignant tumors involving the anterior skull base arise from the respiratory epithelium or glandular tissues of the paranasal mucosa.1 An overwhelming majority of patients with ethmoid sinus malignancy have locally advanced tumors with skull base invasion. It is not uncommon for these patients to have undergone limited surgical manipulations, such as functional endoscopic sinus surgery and sumbucosal resection, before their referral to a skull base surgical team.2 Lesions of the ethmoid sinuses can be divided into primary and secondary tumors. Primary tumors originate in the ethmoid compartment, whereas secondary tumors invade the skull base from the nasal cavity; maxillary, frontal, and sphenoid sinuses; or the skin (Fig. 15.1). Rarely, these tumors originate in the globe, brain, meninges, or infratemporal fossa (Fig. 15.2). Neoplasms arising from the nasal cavity, nasopharynx, paranasal sinuses, and other structures that are in proximity to the anterior base of the skull can interrupt the continuity of the cranial valet, causing cerebrospinal fluid (CSF) leak and pneumocephalus (Fig. 15.3). Primary ethmoid tumors usually invade via the route of least resistance, which includes the sphenoid sinus and nasopharynx posteriorly and the nasal cavity and maxillary sinus inferiorly. Other routes of least resistance are the lamina papyracea (medial orbital wall) and cribriform plate. Primary ethmoid tumors can invade the dura or brain via direct extension through the fovea ethmoidalis (the roof of the ethmoids) and cribriform plate or involve the orbit via lateral extension through the lamina papyracea (Fig. 15.4). Tumors in this area can be of ectodermal, endodermal, or mesodermal origin (Tables 15.1 and 15.2). Tumors of the ethmoids and anterior skull base generally originate from the sinonasal mucosa (i.e., the schneiderian epithelium). The most common of malignant neoplasms in this group is squamous cell carcinoma (SCC), and the most common benign tumor is inverted papilloma. Other carcinomas of the nasal mucosa include sinonasal undifferentiated carcinoma, adenocarcinoma, and mucosal melanoma. Salivary gland tumors are derived from the minor salivary glands of the paranasal mucosa and are usually of malignant origin. Adenoid cystic carcinoma and mucoepidermoid carcinoma are the most common of these tumors. Figure 15.1 Primary and secondary tumors of the ethmoid sinuses. (A) Coronal magnetic resonance imaging (MRI) with gadolinium showing primary osteosarcoma of the ethmoid sinuses, with invasion into the nasal cavity. (B) MRI showing juvenile angiofibroma of the maxillary sinus, with secondary invasion into the ethmoid sinuses. Figure 15.2 (A) Magnetic resonance imaging showing adenocarcinoma originating in the right orbit with invasion into the anterior skull base. (B) Infratemporal fossa involvement of rhabdomyosarcoma. Figure 15.3 (A) Coronal magnetic resonance imaging and (B) axial computed tomography showing osteoma originating in the orbital roof, causing cerebrospinal fluid leak and pneumocephalus. Figure 15.4 (A) Recurrent esthesioneuroblastoma with orbital invasion. (B) High-grade sarcoma with massive brain invasion. Table 15.1 Benign Pathologies of Ethmoid Sinus and Anterior Base of Skull
Ethmoid and Anterior Skull Base Neoplasms
Epidemiology
Routes of Spread
Pathology
Tumors Originating from the Sinonasal Epithelium
Papilloma |
Pleomorphic adenoma |
Dermoid |
Fibroma |
Chondroma |
Osteoma |
Neurofibroma |
Vascular and lymphatic malformations |
Nasal glioma |
Schneiderian papilloma: inverted, papillary, cylindrical |
Angiofibroma |
Fibrous dysplasia |
Ossifying fibroma |
Giant cell tumor |
Adapted from reference 8.
Table 15.2 Malignant Pathologies of Ethmoid Sinus and Anterior Base of Skull
Squamous cell carcinoma |
Basaloid squamous |
Adenosquamous |
Adenoid cystic carcinoma |
Mucoepidermoid carcinoma |
Adenocarcinoma |
Mucosal melanoma |
Olfactory neuroblastoma (esthesioneuroblastoma) |
Sinonasal undifferentiated carcinoma |
Chordoma |
Chondrosarcoma |
Osteogenic sarcoma |
Fibrosarcoma |
Malignant fibrous histiocytoma |
Hemangiopericytoma |
Angiosarcoma |
Rhabdomyosarcoma |
Lymphoma |
Plasmacytoma |
Metastatic |
Bone and Fibrous Tumors
Another group of tumors are the ones that originate in the bony structures of the craniofacial skeleton. These bony lesions include benign conditions, such as fibrous dysplasia, osteoma, and ossifying fibroma, as well as malignant neoplasms, such as osteosarcoma (Fig. 15.5).
Vascular Tumors
Vascular tumors include angiofibroma, paraganglioma, arteriovenous malformation, and hemangioma, all of which are benign conditions (Fig. 15.6). Malignant vascular tumors are rare, and they include hemangiopericytoma, malignant paraganglioma, and angiosarcoma.
Tumors of Muscle and Nerve Origin
Tumors that are derived from muscle tissue are mainly malignant, and the most representative of this group is rhabdomyosarcoma. Common benign nerve cell tumors include schwannoma and neurofibroma, which usually arise in cranial nerves. The malignant tumors in this group are esthesioneuroblastoma and malignant peripheral nerve sheath tumor. Chordoma and chondrosarcoma are malignant soft-tissue tumors that usually arise from the clivus. Head and neck tumors are notorious for their ability to invade nerves. Adenoid cystic carcinomas, sinonasal SCC, and SCC of the skin are among the most common neurotrophic tumors in this group (Fig. 15.7). Tumors that infiltrate the base of the skull via nerve dissemination can eventually involve the dura and brain.3
Presenting Signs and Symptoms
Signs and symptoms can often be misleading and initially interpreted as infectious and benign disease. Because early detection is probably the most important factor in improving prognosis, a high degree of suspicion is necessary for any symptom suggestive of a growing tumor in the nasal cavity and sinuses. The most common signs and symptoms of malignant neoplasms are listed in Table 15.3. There may also be locoregional neck metastases in fewer than 10% of the patients with malignant tumors. The physical examination should always include a fiberoptic endoscopic evaluation of the nose, sinuses, nasopharynx, and oropharynx. Special attention should also be paid to the presence of facial asymmetry, proptosis, serous otitis media, cranial nerve palsies, and suspicious neck nodes (Fig. 15.8).
Radiological Evaluation
All patients with suspected craniofacial neoplasm should undergo a radiological evaluation. Imaging is critical for the evaluation of location, size, and extent of disease and for differential diagnosis. Imaging is also important for guiding a transnasal biopsy. Computed tomography (CT) and magnetic resonance imaging (MRI) are the modalities of choice for staging and follow-up of skull base tumors. The main advantage of CT scans is their superiority in delineating the architecture of the bones. Adding contrast enhancement to the study increases tumor definition from adjacent soft tissue. Bone destruction and soft-tissue invasion suggest an aggressive behavior pattern. Widening of the foraminas in the base of the skull can indicate perineural spread. The main advantage of MRI is its supremacy in delineating among soft-tissue structures, especially muscles, brain, and dura. Moreover, MRI best evaluates brain, cavernous sinus, carotid artery, perineural invasion (Fig. 15.9), and intraorbital invasion (Fig. 15.10). Dural thickening or enhancement may suggest dural involvement. Perhaps one of the most significant advantages of MRI is its ability to distinguish the tumor from retained secretions secondary to obstruction of sinus drainage. This is best demonstrated with a T2-MRI scan (Fig. 15.11). Positron emission tomography-CT is used for further assessment of the patient’s metastatic status (Fig. 15.12). Its superiority in the delineation of regional and distant metastases has made MRI a highly valuable tool both in the preoperative evaluation and for follow-up because it can help distinguish between postoperative changes and tumor recurrence.
Tissue Diagnosis
Tissue diagnosis is crucial for the individual tailoring of treatment and should always be performed after a proper imaging work-up. Tissue is usually obtained by means of endoscopic biopsy under local anesthesia. An adequate specimen of the tissue should be obtained, with care being taken to avoid crushing it. If the lesion is suspected for being of a lymphoproliferative nature, the fresh tissue should be immersed in saline rather than fixed in formalin. Biopsy should be avoided if the nasal mass is suspected to be as an encephalocele, because the procedure can lead to CSF leak and meningitis. Similarly, biopsy is contraindicated for suspected vascular lesions, such as juvenile angiofibromas, hemangiopericytomas, and hemangiomas. The biopsy specimen should be examined by a pathologist who is an expert in the field of head and neck cancer (HNC).
Tailoring of Treatment
Malignant tumors of the ethmoids and anterior skull base are almost always treated by surgery. Exceptions are lymphomas and small cell carcinomas, which are managed by chemoradiation. Surgery is contraindicated in highly malignant neoplasms when the tumor infiltrates the internal carotid artery or cavernous sinus, and when there is evidence of high volume disease in the brain parenchyma (Fig. 15.13). The goals of surgery are complete tumor resection and preservation of function. The classical resections of malignant tumors of the anterior skull base and ethmoids are performed via transfacial or transcranial open approaches. Recent developments in minimally invasive modalities have led to the popularization of endoscopic surgery for resection of benign and malignant tumors of the anterior skull base and paranasal sinuses.4
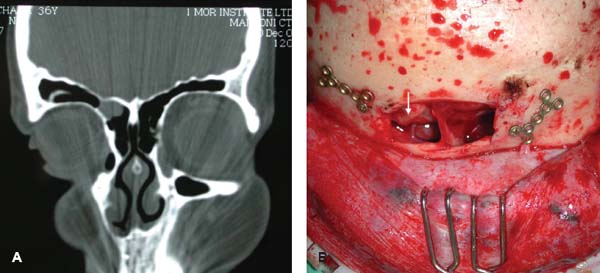
Figure 15.5 Osteoma of the right frontal bone. (A) Coronal computed tomography. (B) Intraoperative view. The arrow indicates the osteoma.



