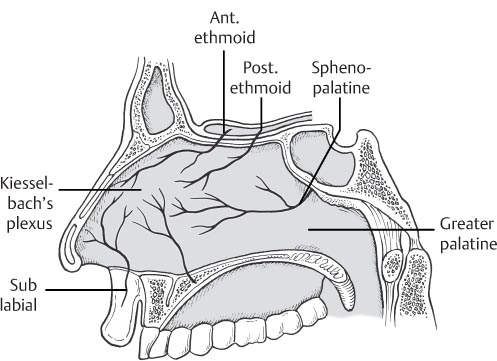
29 Epistaxis The blood supply of the nose comes from branches of both the internal and external carotid artery systems, and there are multiple anastomoses between the two systems. Knowledge of the nasal cavity’s blood supply affects how epistaxis is diagnosed and treated. Fig. 29.1 Arterial supply of the lateral nasal wall. — Lateral branches of the SPA (or posterior nasal artery): These are terminal branches of the SPA supplying the lateral nasal wall and the middle and inferior turbinates. — Septal branch of the SPA: This branch crosses the anterior face of the sphenoid (inferior to the ostia) before branching onto the posterior septum. — Woodruff region: Throughout the nose there are several areas of anastomosis between the many arteries that supply the mucosa. The Woodruff region, also known as the nasopharyngeal plexus, lies on the posterolateral nasal wall in the region of the inferior meatus (between the inferior turbinate and nasal floor). It comprises vessels from the pharyngeal and posterior nasal arteries. — Septal branch of SPA: After the SPA has entered the nasal cavity and given off branches to the lateral nasal wall, the septal branch then continues across the sphenoid face to become the major blood supply to the posterior septum. — Greater palatine artery: The descending palatine artery is a branch of the SPA and passes through the palatine canal where it becomes the greater palatine artery. It then passes through the incisive canal to supply the nasal floor and anteroinferior septum. Fig. 29.2 Arterial supply of the septum. — Little area: The Little area, also known as the Kiesselbach plexus, is an area of anastomosis on the anterior nasal septum. It is the major area of anastomosis between the external and internal carotid artery blood supply to the nose. The vessels in Little’s area come from the SPA, greater palatine, anterior ethmoidal, posterior ethmoidal, and nasal branches of the superior labial arteries. — Woodruff plexus of the posterior septum: Some authors consider the Woodruff plexus as a region of the posterior septum where ethmoid artery branches anastomose with the septal branches of the SPA. — Illicit intranasal drug use — Trauma: external (eg, blunt trauma, fracture) and internal (eg, finger manipulation) — Recent nasal surgery — Always use personal protective equipment (eye protection, gloves, mask, etc.). — Anterior rhinoscopy
 Anatomy
Anatomy
 Lateral nasal wall (Fig. 29.1)
Lateral nasal wall (Fig. 29.1)
 Anterior ethmoidal artery: The anterior ethmoidal artery branches off the ophthalmic, which is the first branch of the internal carotid artery. The anterior ethmoidal artery enters the anterior ethmoidal foramen, which is ~14 to 22 mm posterior to the anterior crest of the lacrimal fossa. This is usually at the horizontal plane of the cribriform plate. The vessel then passes just under the skull base across the roof of the anterior ethmoid sinuses. The lateral branch supplies the anterior aspect of the lateral nasal wall. The anterior ethmoidal artery is absent in 7 to 14% of the population.
Anterior ethmoidal artery: The anterior ethmoidal artery branches off the ophthalmic, which is the first branch of the internal carotid artery. The anterior ethmoidal artery enters the anterior ethmoidal foramen, which is ~14 to 22 mm posterior to the anterior crest of the lacrimal fossa. This is usually at the horizontal plane of the cribriform plate. The vessel then passes just under the skull base across the roof of the anterior ethmoid sinuses. The lateral branch supplies the anterior aspect of the lateral nasal wall. The anterior ethmoidal artery is absent in 7 to 14% of the population.
 Posterior ethmoidal artery: The posterior ethmoidal artery is also a branch of the ophthalmic artery. It enters the posterior ethmoidal canal, which is usually located in the frontoethmoid suture, ~10 mm posterior to the anterior ethmoidal canal. The posterior ethmoidal artery has a lateral branch supplying the superior aspect of the lateral nasal wall. The posterior ethmoidal artery is absent in ~31% of the population.
Posterior ethmoidal artery: The posterior ethmoidal artery is also a branch of the ophthalmic artery. It enters the posterior ethmoidal canal, which is usually located in the frontoethmoid suture, ~10 mm posterior to the anterior ethmoidal canal. The posterior ethmoidal artery has a lateral branch supplying the superior aspect of the lateral nasal wall. The posterior ethmoidal artery is absent in ~31% of the population.
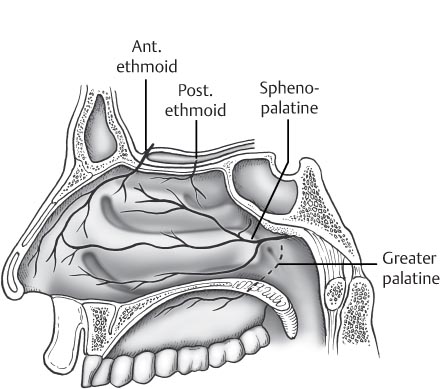
 Ascending pharyngeal artery branches: The ascending pharyngeal artery is a branch of the maxillary artery and supplies the inferoposterior lateral nasal wall.
Ascending pharyngeal artery branches: The ascending pharyngeal artery is a branch of the maxillary artery and supplies the inferoposterior lateral nasal wall.
 Superior labial artery: Another branch by which the external carotid artery provides blood to the lateral nasal wall is the superior labial artery, which is a branch of the facial artery. It provides several nasal branches supplying the anterolateral nasal wall.
Superior labial artery: Another branch by which the external carotid artery provides blood to the lateral nasal wall is the superior labial artery, which is a branch of the facial artery. It provides several nasal branches supplying the anterolateral nasal wall.
 Vascular regions
Vascular regions
 Nasal septum (Fig. 29.2)
Nasal septum (Fig. 29.2)
 Anterior ethmoidal artery: The anterior ethmoidal artery gives off me-dial and lateral branches. The medial branch supplies the anterosuperior nasal septum.
Anterior ethmoidal artery: The anterior ethmoidal artery gives off me-dial and lateral branches. The medial branch supplies the anterosuperior nasal septum.
 Posterior ethmoidal artery: The posterior ethmoidal artery has medial and lateral branches. The medial branch supplies the superior septum.
Posterior ethmoidal artery: The posterior ethmoidal artery has medial and lateral branches. The medial branch supplies the superior septum.
 Sphenopalatine artery (SPA)
Sphenopalatine artery (SPA)
 Superior labial artery: Nasal branches from the superior labial artery enter the nose to supply the anterior septum.
Superior labial artery: Nasal branches from the superior labial artery enter the nose to supply the anterior septum.
 Vascular regions
Vascular regions
 Diagnostic Factors to Consider in Epistaxis
Diagnostic Factors to Consider in Epistaxis
 Location
Location
 Anterior: Anterior epistaxis often originates from Little area (Kiesselbach plexus) on the nasal septum.
Anterior: Anterior epistaxis often originates from Little area (Kiesselbach plexus) on the nasal septum.
 Posterior
Posterior
 Hemoptysis can be the presenting sign of epistaxis, particularly posterior epistaxis.
Hemoptysis can be the presenting sign of epistaxis, particularly posterior epistaxis.
 Hematemesis can also be the presenting sign of epistaxis, particularly posterior epistaxis. Patients with neurological disease involving a decreased gag reflex may be more prone to ingesting large quantities of blood, and patients who are supine for a long period of time (eg, an intubated patient in the intensive care unit) is at increased risk of ingesting or aspirating blood from epistaxis.
Hematemesis can also be the presenting sign of epistaxis, particularly posterior epistaxis. Patients with neurological disease involving a decreased gag reflex may be more prone to ingesting large quantities of blood, and patients who are supine for a long period of time (eg, an intubated patient in the intensive care unit) is at increased risk of ingesting or aspirating blood from epistaxis.
 Frequency
Frequency
 Other factors in history
Other factors in history
 Other bleeding sites: A history of other bleeding, especially mucosal bleeding, can be indicative of a systemic cause of epistaxis.
Other bleeding sites: A history of other bleeding, especially mucosal bleeding, can be indicative of a systemic cause of epistaxis.
 Family history of bleeding
Family history of bleeding
 Medications: There are numerous medications that are associated with epistaxis. Antiplatelet drugs such as aspirin and clopidogrel, warfarin, and nasal sprays may play a role in epistaxis.
Medications: There are numerous medications that are associated with epistaxis. Antiplatelet drugs such as aspirin and clopidogrel, warfarin, and nasal sprays may play a role in epistaxis.
 Physical examination
Physical examination
 Airway, breathing, and circulation: always important first steps in any patient with active bleeding or trauma
Airway, breathing, and circulation: always important first steps in any patient with active bleeding or trauma
 Nasal exam
Nasal exam
 Remove all blood clots.
Remove all blood clots.
 Use topical decongestant for visualization and to slow or stop bleeding. Placement of a cotton pledget with a topical vasoconstrictor may be needed to allow visualization.
Use topical decongestant for visualization and to slow or stop bleeding. Placement of a cotton pledget with a topical vasoconstrictor may be needed to allow visualization.


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


