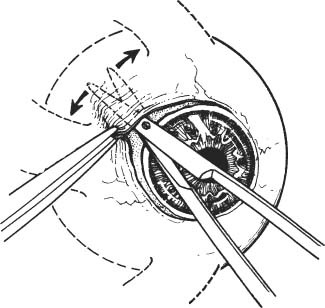
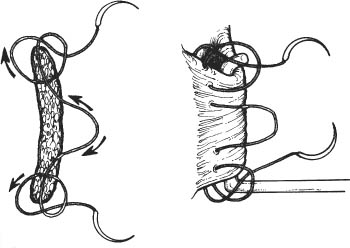
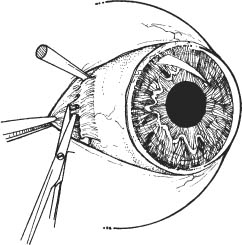
59 See Chapter 58. See Chapter 3. 1. Treat any infectious processes as necessary. 2. If possible, discontinue aspirin and nonsteroidal anti-inflammatory agents for 10 days prior to surgery. Discontinue warfarin 2–3 days preoperatively, if medically possible. 3. Query patient about bleeding tendencies. A useful screening question is asking if the patient had unusual bleeding after dental extraction. Obtain hematological evaluation if bleeding tendency is suspected. 1. Determine method to be used for enucleation: a. Technique I: Silicone or methylmethacrylate sphere b. Technique II: Medpor sphere Note: Text will indicate where techniques vary. 2. General anesthesia in most cases. 3. Verify eye to be enucleated. 4. Prep and drape in sterile manner. 5. Place lid speculum. 6. Perform 360 degree limbal peritomy taking care to preserve all conjunctiva (Westcott scissors). Figure 59.1 7. Bluntly spread between rectus muscles in all quadrants (Fig. 59.1). a. Use Westcott or Stevens scissors to bluntly buttonhole through the Tenon capsule down to bare sclera. b. Aim scissors 45 degrees between rectus muscles. c. Spread scissors. Figure 59.2 8. Isolate medial and lateral rectus muscle with muscle hooks (Fig. 59.2). 9. Use Q-tip or scissors to conservatively strip the Tenon capsule. Figure 59.3
Enucleation
Indications
 Intraocular tumors
Intraocular tumors
 Blind eyes following severe penetrating injuries
Blind eyes following severe penetrating injuries
 Blind eyes with recalcitrant infections
Blind eyes with recalcitrant infections
 Blind, painful eyes unresponsive to medical treatment
Blind, painful eyes unresponsive to medical treatment
Preoperative Procedures
Instrumentation
 Lid speculum
Lid speculum
 Toothed forceps
Toothed forceps
 Sutures (6–0 Vicryl, 6–0 plain, 5–0 Vicryl)
Sutures (6–0 Vicryl, 6–0 plain, 5–0 Vicryl)
 Needle holder
Needle holder
 Cautery
Cautery
 Scissors (Westcott, Stevens)
Scissors (Westcott, Stevens)
 Muscle hooks
Muscle hooks
 Spherical implant (silicone or methylmethacrylate for Technique One and Medpor SST implant for Technique II; see below)
Spherical implant (silicone or methylmethacrylate for Technique One and Medpor SST implant for Technique II; see below)
 Sizer set of spheres
Sizer set of spheres
 Methylmethacrylate conformer
Methylmethacrylate conformer
Operative Procedures
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


