Endoscopy
Endoscopic assessment of the nose and nasopharynx has become an integral part of the evaluation of patients with sinonasal disorders. Anterior rhinoscopy is simple to perform in most patients and is considered part of the basic head and neck examination. When distal pathology is suspected, pediatric endoscopes are often employed for the accurate evaluation of the patient’s complaint. Moreover, recent technological advances have allowed for photographic and video documentation of pathology, facilitating discussion with the family and other practitioners.
30-1 Rhinoscopy
Indications
Anterior rhinoscopy is part of the basic head and neck physical examination.
Preoperative Evaluation
No specific evaluations are required for rhinoscopy.
Operative Technique
1. No anesthetic or vasoconstricting substance is necessary for limited anterior rhinoscopy.
2. The child is in the upright position seated in a chair or in the caretaker’s lap.
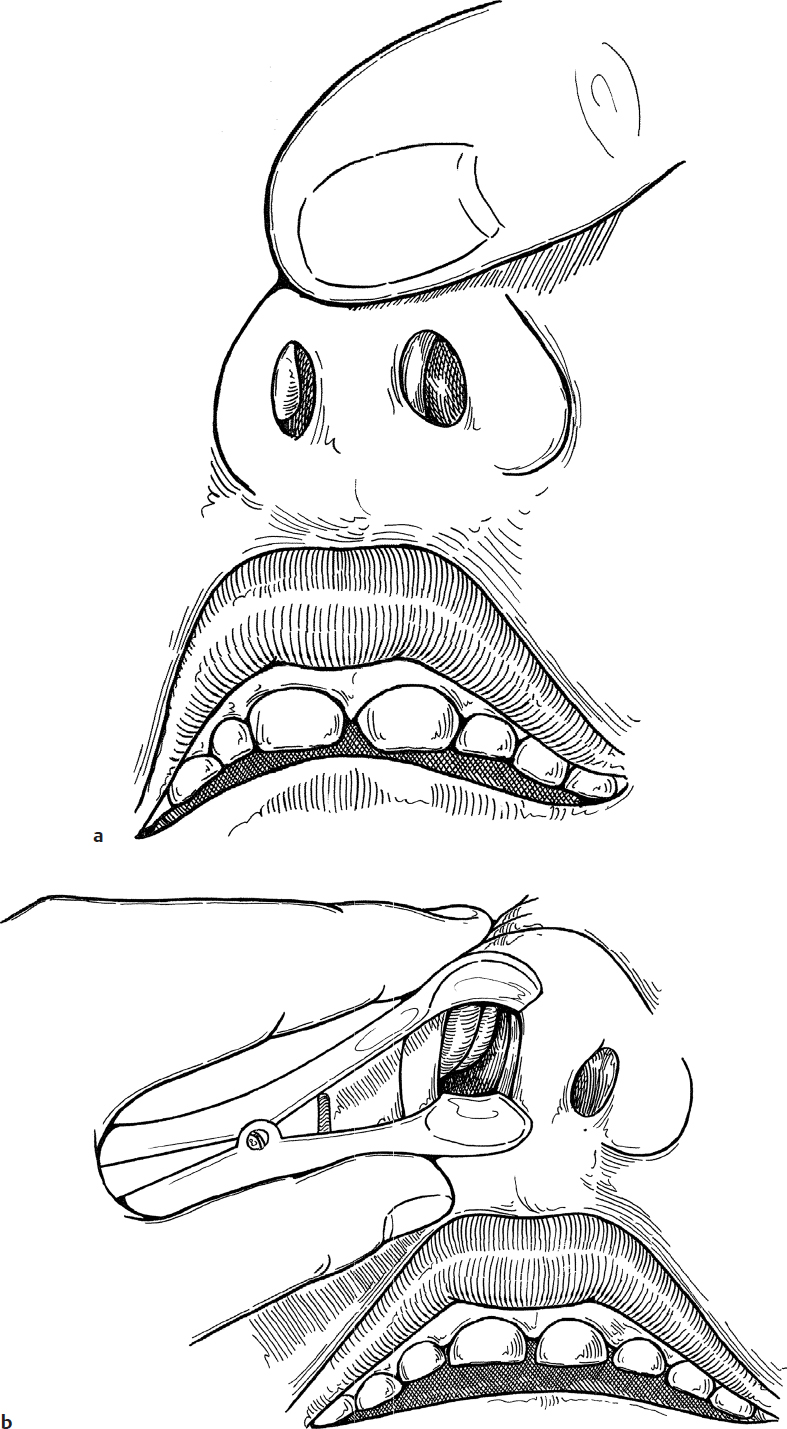
3. The child’s mobile nasal tip is gently elevated with the examiner’s thumb as a directed light source is shined into the nasal cavity. In this way, the anterior nasal septum, nasal vestibule, and the inferior and, occasionally, the middle turbinate can be examined easily (Fig. 30.1a).
4. If redundant or collapsible tissue or nasal hairs prevent adequate visualization, a standard nasal speculum can be inserted gently into the nasal vestibule and the internal structures visualized.
5. Care must be taken to stabilize the instrument with the examiner’s right forefinger on the patient’s nasal tip so that the instrument will follow any movements of the child’s head (Fig. 30.1b). An otoscope with a large speculum may be substituted for the nasal speculum.
6. If examination of the more posterior aspect of the nasal cavity is needed, posterior rhinoscopy can be performed utilizing a straight telescope. Topical anesthesia and vasoconstriction are obtained using cotton pledgets soaked in 4% cocaine (alternately, any combination of a topical vasoconstrictor and local anesthetic may be used). The telescope can then be advanced into the nasal cavity to inspect the deeper aspects of the turbinates and the nasal septum (Fig. 30.1c). Rigid telescopes are available in different viewing angles so that the entire nasal cavity can be examined.
7. A flexible telescope may be inserted and angulated in different directions to view the entire nasal cavity (Fig. 30.1d).
Complications
1. Epistaxis
2. Mucosal abrasion