Purpose
To assess the feasibility and efficacy of endoscopic transnasal removal of cavernous hemangiomas of the optic canal.
Design
Retrospective, noncomparative case series.
Methods
Eleven consecutive patients (11 eyes) with cavernous hemangioma of the optic canal underwent endoscopic trans-ethmoidal-sphenoidal removal of the tumor at the Eye Hospital of Wenzhou Medical University from January 2009 to March 2016. In each case, the indication for surgery was decreased visual acuity due to the tumor. The removal was believed to be complete if the tumor was removed en bloc during the surgery. A mucoperiosteal flap was used to cover the defect in the optic nerve sheath after tumor removal. The tumor was pathologically confirmed to be cavernous hemangioma after surgery. The mean follow-up time was 9.9 ± 5.5 months. Visual acuity before and after surgery was compared.
Results
All tumors were completely removed by the endoscopic approach. The best-corrected visual acuity (BCVA) improved after surgery in all patients. The mean preoperative BCVA was 6/30 (95% confidence interval [CI] 6/60–6/20) and the mean postoperative BCVA was 6/10 (95% CI 6/12–6/7.5). All patients showed cerebrospinal fluid rhinorrhea, which resolved with strict bed rest. Other complications included hyposmia in 2 patients; nasal bleeding in 3 patients, which resolved spontaneously; and temporary headache.
Conclusions
Endoscopic trans-ethmoidal-sphenoidal approach is a feasible option for cavernous hemangiomas of the optic canal.
Cavernous hemangiomas are one of the most common orbital tumors in adults. According to the International Society for the Study of Vascular Anomalies classification, cavernous hemangiomas should be classified as low-flow venous malformations. Most of them are located in the middle third of the orbit and those located in the optic canal are very rare. The bony structure of the optic canal offers little space for tumor growth. A small lesion can compress the optic nerve, leading to vision loss. In 1984, Costa e Silva and Symon first recognized 2 cases of cavernous hemangioma of the optic canal. Both patients presented with vision loss and headache. The tumor was not suspected preoperatively and was discovered on orbitocranial exploration. Unfortunately, there was no improvement in vision after removal of the tumor in either case. In 1994, Sato and associates discussed computed tomography (CT) and magnetic resonance imaging (MRI) appearance in a single case report and the tumor was removed by craniotomy without mention of surgical outcome. Schick and associates also reported 1 case of canalis opticus cavernomas removed by pterional intradural approach, but no visual improvement was gained after surgery. In recent years, we have developed the endoscopic technique to remove these lesions through the trans-ethmoidal-sphenoidal approach. In this study, we report 11 cases of cavernous hemangiomas of the optic canal treated via this approach.
Methods
We reviewed the records of all patients between January 1, 2009 and March 31, 2016 who underwent endoscopic operation for cavernous hemangiomas of the optic canal at the Eye Hospital of Wenzhou Medical University; altogether, 11 patients were identified. Charts were reviewed for clinical history, surgical approach, outcome, and radiologic images. The ophthalmologic examinations before and after surgery included best-corrected visual acuity (BCVA), visual field, pupil reflex, motility, and complete status of the anatomy of both eyes. High-resolution computed tomography (HRCT) and MRI with gadolinium of the orbit were performed preoperatively in all cases. Clinical diagnosis was based on symptoms and signs together with radiologic images. Resected tumors further pathologically confirmed the diagnosis of cavernous hemangiomas. Indications for operation were clinical symptoms of visual decline that were attributable to the tumor. All surgeries were performed under general anesthesia by 1 single surgeon (W.W.) using endoscopic trans-ethmoidal-sphenoidal approach. Written informed consent was obtained from every patient before surgery. The study adhered to the tenets of the Declaration of Helsinki and Ethics Committee approval was obtained.
Surgical Procedures
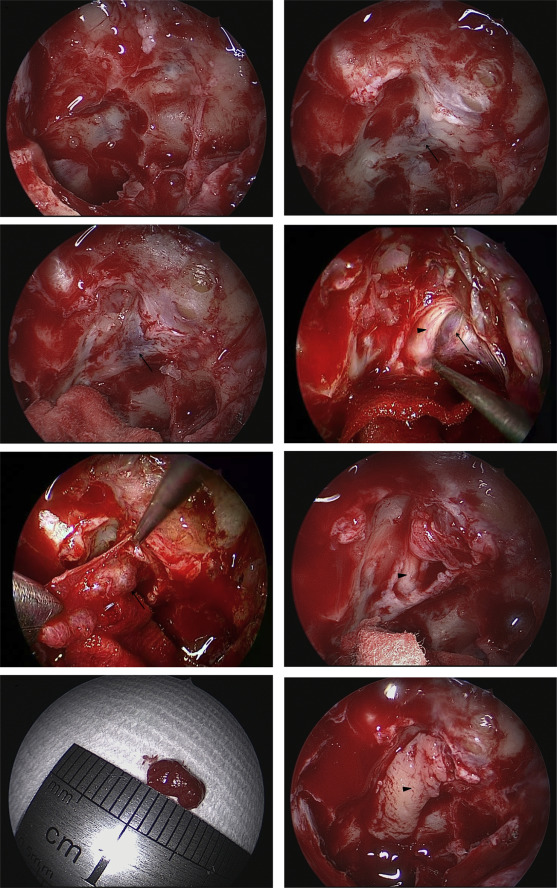
A standard endoscopic transnasal ethmoidectomy was carried out using a 4.0-mm, 45-degree endoscope (Karl Storz, Tuttlingen, Germany), after which the sphenoidal sinus was abundantly opened by removing its anterior wall. The optic canal and its adjacent characteristic structures, such as the anterior cranial base, orbital apex, and internal carotid artery, were identified. Then the sinus mucosa covering the optic canal was meticulously peeled off with a small sickle knife and the purple bulge visible through the medial bony wall of the optic canal was the exact location of the small lesion. Most of the medial bony wall of the optic canal from the entrance of the orbital apex to the cranial cavity was thinned using a microdrill (drill bit: diamond/15 degree/round shape in 2.9 mm diameter, integrated power console; Medtronic Inc, Fort Worth, TX, USA) and removed carefully to fully expose the tumor covered by the optic sheath. Then the optic sheath was slightly and carefully incised with a sharp #9 MVR knife about 1–2 mm away from the tumor from 4 directions (superior, inferior, anterior, posterior). After that the surgeon dissected the optic sheath covering the tumor with the small sickle knife or the #9 MVR knife while an assistant strained the optic sheath with a long thin forceps. Once the optic sheath was excised, the well-circumscribed purple encapsulated lesion, as well as the white optic nerve, was visible and the cerebrospinal fluid flowed out. The surgeon further separated the tumor from the arachnoid by blunt dissection from posterior to anterior while the assistant pulled the optic sheath medially and superiorly away from the optic nerve. During the dissection, the pupil of the operated eye was closely observed. If the pupil dilated during this procedure, which indicated possible optic nerve injury by mechanical damage or vascular compromise, any traction was released immediately and precise dissection of the tumor must be relocated. There was usually a clear demarcation of the cavernomas facilitating the separation from the optic nerve. The lesion was dissected circumferentially and removed en bloc from the optic nerve. After tumor resection, the optic nerve was clearly visible with partial absence of the optic sheath, accompanied by the cerebrospinal fluid gushing out. The final step was to reconstruct the optic nerve sheath defect with a mucoperiosteal flap, which was cut from the ipsilateral middle turbinate and deprived of bony tissue. The optic nerve sheath defect was covered by the mucoperiosteal flap with the epithelial side facing the sinus, preventing outflow of the cerebrospinal fluid. Finally, the surgical field was gently covered with 1–2 pieces of gelatin sponge soaked in dexamethasone (5 mg/2 mL) and mouse-derived nerve growth factor (30 mg/mL) (Staidson Biopharmaceuticals Co, Beijing, China) ( Figure 1 ) ( Supplemental Video available at AJO.com ).
Postoperative management included intravenous methylprednisolone (500 mg) for 3 days and intravenous broad-spectrum antibiotics for 5 days. The patients were positioned to lie in bed for 4–7 days after surgery, in a 30-degree tilt position with head up and feet down. Nose-blowing or strenuous activity was prohibited for the first 2 weeks after surgery. Because all the tumors had a clear demarcation and were removed en bloc during the surgery, the removal was believed to be complete and no further imaging examination was conducted.
Results
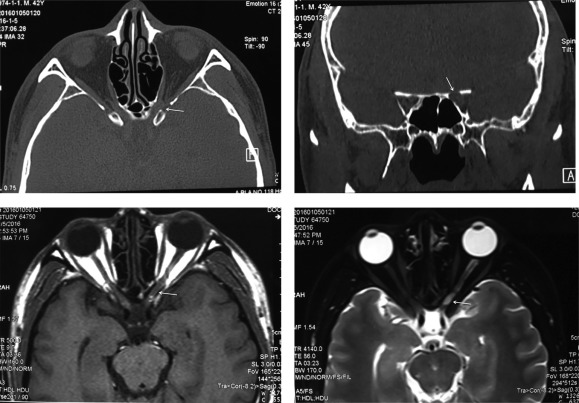
This case series consisted of 11 patients with small cavernous hemangiomas of the optic canal who underwent surgery between January 2009 and March 2016. The population was composed of 8 men and 3 women with mean age of 43.5 ± 7.1 years (range, 35–57 years) and followed up for 9.9 ± 5.5 months (range, 3–24 months). All the patients had insidious onset and complained of slowly progressive visual decline with an average onset of 11.5 ± 10.1 months (range, 1–36 months) before presentation. The preoperative BCVA ranged from 6/300 to 6/12. On ophthalmologic examination, the pupil of the affected eye was dilated with a relative afferent pupillary dysfunction (RAPD) and the optic disc was pale with a clear margin. All patients showed color vision alteration and visual field defect, though no one complained of subjective symptoms. On HRCT, the tumor could be noticed as a roundish, slightly higher-density mass accompanied by local enlargement of the optic canal. MRI showed a better visualization of an iso-intensity mass on T1-weighted sequences and a high-intensity mass on T2-weighted sequences, with enhancement irregular in modality and inconsistent in density ( Figure 2 ). All tumors were removed completely and the average operation time was 2.06 ± 0.58 hours. All patients gained BCVA improvement after surgery, with postoperative BCVA ranging from 6/24 to 6/6. The mean preoperative BCVA was 6/30 (95% CI 6/60–6/20) and the mean postoperative BCVA was 6/10 (95% CI 6/12–6/7.5). The color vision and visual field showed partial recovery in every patient while the appearance of the optic disc and positive RAPD remained the same ( Table ).
| Patient No. | Sex | Age (y) | History (m) | Visual Decline Before Surgery | BCVA | Optic Disc | RAPD | Color Vision | Visual Field | Tumor Size (cm) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Preop | Postop | Preop | Postop | Preop | Postop | Preop | Postop | Preop | Postop | ||||||
| 1 | M | 38 | 8 | Yes | 6/20 | 6/7.5 | Pale | Pale | + | + | Abnormal | Improved | Irregular defect | Improved | 0.5×0.3×0.3 |
| 2 | F | 47 | 24 | Yes | 6/30 | 6/10 | Pale | Pale | + | + | Abnormal | Improved | Irregular defect | Improved | 0.6×0.4×0.5 |
| 3 | M | 53 | 36 | Yes | 6/36 | 6/10 | Pale | Pale | + | + | Abnormal | Improved | Irregular defect | Improved | 0.4×0.3×0.5 |
| 4 | M | 42 | 4 | Yes | 6/300 | 6/24 | Pale | Pale | + | + | Abnormal | Improved | Irregular defect | Improved | 0.8×0.5×0.4 |
| 5 | F | 36 | 12 | Yes | 6/12 | 6/7.5 | Pale | Pale | + | + | Abnormal | Improved | Irregular defect | Improved | 0.3×0.4×0.2 |
| 6 | M | 40 | 5 | Yes | 6/24 | 6/6 | Pale | Pale | + | + | Abnormal | Improved | Irregular defect | Improved | 0.5×0.3×0.4 |
| 7 | M | 48 | 11 | Yes | 6/30 | 6/8.5 | Pale | Pale | + | + | Abnormal | Improved | Irregular defect | Improved | 0.6×0.4×0.4 |
| 8 | F | 44 | 1 | Yes | 6/60 | 6/12 | Pale | Pale | + | + | Abnormal | Improved | Irregular defect | Improved | 0.7×0.3×0.4 |
| 9 | M | 38 | 7 | Yes | 6/20 | 6/10 | Pale | Pale | + | + | Abnormal | Improved | Irregular defect | Improved | 0.5×0.4×0.2 |
| 10 | M | 35 | 6 | Yes | 6/12 | 6/6 | Pale | Pale | + | + | Abnormal | Improved | Irregular defect | Improved | 0.3×0.4×0.3 |
| 11 | M | 57 | 12 | Yes | 6/30 | 6/12 | Pale | Pale | + | + | Abnormal | Improved | Irregular defect | Improved | 0.5×0.4×0.2 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


