Purpose
To determine the indications for the addition of a transcaruncular approach along with detachment of the medial rectus muscle during the removal of small apical cavernous hemangiomas using an endoscopic transethmoidal approach.
Design
Retrospective, noncomparative case series.
Methods
Multicenter study of 12 patients with apical orbital tumors removed using an endoscopic transethmoidal approach. The decision to detach the medial rectus muscle with the addition of a transcaruncular approach was made during surgery for tumors largely lateral to the medial rectus muscle. Tumors adjacent to the medial orbital wall were removed via an endoscopic transethmoidal approach alone.
Results
Seven tumors were removed via an endoscopic transethmoidal approach combined with medial rectus muscle detachment, whereas 5 patients underwent removal without detachment of the medial rectus. All patients had visual impairment. Complete excision of the hemangiomas was achieved in all patients and tumor size ranged from 6 × 5 mm to 20 × 12 mm. The mean postoperative follow-up time was 11.8 ± 4.3 months. At final follow-up, the best-corrected visual acuity improved in 11 patients. Three patients had transient horizontal diplopia resulting from partial paralysis of the medial rectus muscle after detachment during surgery.
Conclusions
The endoscopic transethmoidal approach with or without medial rectus detachment is a promising approach for selected small cavernous hemangiomas located at the deep medial orbital apex. Detachment of the medial rectus muscle can be a useful technique for tumors located largely lateral to the medial rectus muscle. Further studies will be required to demonstrate the safety and efficacy of this technique.
A variety of approaches have been used in the management of orbital cavernous hemangiomas. However, removal of small cavernous hemangiomas located in the deep orbital apex remains problematic because of the higher risks of collateral damage. Recently, an endoscopic transethmoidal (or transsphenoidal) approach has been reported for extraconal or intraconal tumors, or both, in a few cases. The endoscopic transethmoidal approach is suitable primarily for selected well-defined extraconal and intraconal lesions located medial or inferomedial to the optic nerve, preferably adjacent to the medial orbital wall. The presence of significant expansion of the medial orbital wall and extension into the sphenoid or ethmoid sinus, or both, often facilitates transnasal removal in these cases. However, the literature on this approach is limited for apical hemangiomas, and we are unaware of any previous reports addressing the need for medial rectus muscle detachment in selected intraconal cases and could find no reference to it in a computerized search of PubMed. Hence, in this study, we set out to analyze our experience with an endoscopic transethmoidal approach for removal of small cavernous hemangiomas located in the orbital apex and the indications for the addition of a transcaruncular approach with medial rectus muscle detachment.
Methods
The study adhered to the tenets of the Declaration of Helsinki and was approved by the ethics committees of the Eye Hospital of Wenzhou Medical College, Quzhou People’s Hospital, the Second People’s Hospital of Zhengzhou, and the Royal Adelaide Hospital for retrospective review of patient data. Written consent was obtained from all patients before surgery. The records of 9 patients evaluated at the Eye Hospital of Wenzhou Medical College (Patients 1 through 6), the Ophthalmic Department of the Quzhou People’s Hospital (Patients 7 and 8), and the Second People’s Hospital of Zhengzhou (Patient 9) for surgical resection of small cavernous hemangiomas from January 2008 through December 2011 were reviewed retrospectively. The records of 3 patients managed at the Royal Adelaide Hospital between January 2008 and February 2012 also were analyzed. Computed tomography of the orbit (axial and coronal planes, 1.0- or 1.5-mm thickness of continuous sections), magnetic resonance imaging with gadolinium, or both were performed before surgery in all cases for diagnosis and determination of the location of the tumors. Preoperative and postoperative data on best-corrected visual acuity (BCVA), on pupillary dysfunction, for visual fields (Humphrey static threshold automated perimetry, Carl Zeiss Meditec Inc., Dublin, California, USA), and from dilated fundus examination were analyzed. All surgeries at Wenzhou Medical College were performed by a single surgeon (W.W.), and those at the Royal Adelaide Hospital were performed by a single surgeon (D.S.).
Surgical Procedure
All procedures were performed under general anesthesia. The 3 cases from Adelaide underwent controlled hypotensive anesthesia with a laryngeal mask. A standardized endoscopic transnasal ethmoidectomy was performed using a 4.0-mm, 45-degree endoscope (Karl Storz, Tuttlingen, Germany). The lamina papyracea was skeletonized and exposed to the orbital apex as far as necessary before being elevated and removed from the periorbita by a microcurette or a Freer elevator (New Direction Medical Optic Instrument Co., Dezhou, China) until the junction between the minor wing of sphenoid bone and the optic canal was visualized. The anterior extent of the bone removal was dependent on the location of the hemangioma and the anticipated exposure required.
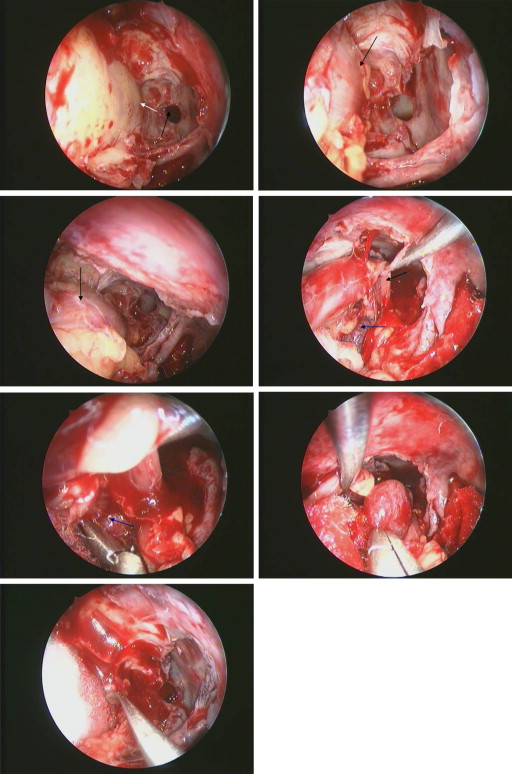
In cases where the hemangioma was adjacent to the medial wall and was easily accessible from below the medial rectus muscle or was situated between the medial rectus muscle and the wall, the medial rectus muscle was not detached and the entire procedure was completed endonasally ( Figure 1 ). In these cases, the anterior extent was posterior to the posterior lacrimal crest in some patients. Two longitudinal periorbital incisions parallel to the medial rectus muscle were made superiorly and inferiorly from orbital apex anteriorly to just behind the posterior border of the lacrimal sac with a sharp sickle knife. The posterior and anterior limits of the incisions then were connected with 2 vertical incisions and the periorbita was removed to leave a rectangular window. The extent of the periorbital incisions anteriorly was dependent on whether there was likely to be a need for retraction of the medial rectus muscle, because this is facilitated with the majority of the length of the muscle exposed. If orbital fat prolapsed into the surgical field to obscure visualization of the hemangioma, then the extraconal orbital fat was excised carefully. This was more common if the hemangioma was located in the medial intraconal space lateral to the medial rectus. If required, the extraconal fat between the periorbita and the posterior medial rectus muscle was excised with a special manual cutting instrument (New Direction Medical Optic Instrument Co, Ltd, Dezhou, Shandong, China) to expose the far posterior medial rectus muscle.
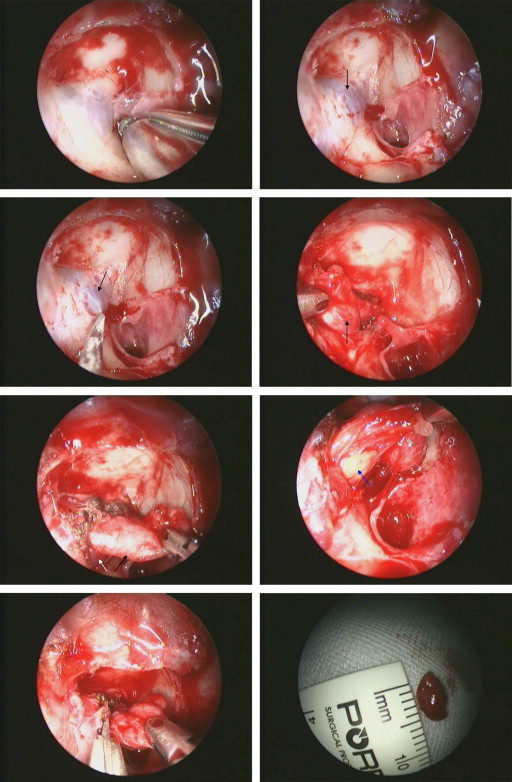
If the hemangioma was located lateral to the medial rectus, then the medial rectus muscle tendon was detached from the globe via a transconjunctival incision to enable better manipulation of the medial rectus muscle at the orbital apex ( Figure 2 ). The decision to detach the medial rectus was made during surgery if the hemangioma was lateral to the muscle and adequate endonasal retraction of the rectus was difficult. A blunt ribbon retractor was inserted through the surgical nose and into the ethmoid sinus and was placed under the inferior border of the posterior medial rectus muscle to retract it superomedially to expose the orbital apex. Alternatively, retraction was achieved through a transcaruncular incision using thin malleable brain retractors or squint hooks, and a 3- or 4-hand surgical technique was used to enable dissection of the hemangioma. After the hemangioma was identified, long, thin grasping forceps were used to grasp the capsule of the lesion and then to retract it gently both medially and inferiorly. If there was adherence to the surrounding tissue, another point of the capsule proximate to the adherence was grasped and then cautiously was pulled medially to release it. If there was significant adherence, then a bimanual technique with the assistant holding the scope and retractor and the endonasal surgeon using the forceps and blunt dissector was used. If there was significant adhesion on the posterolateral aspect of the hemangioma, then the primary surgeon dissected this area via the transcaruncular route while medial retraction into the ethmoid sinus was provided by the assistant via the endonasal approach. Finally, the medial rectus muscle, if detached, was reattached using 6-0 absorbable sutures. If the bony defect was greater than half the medial wall, this was reconstructed with a thin Medpor (Stryker Leibinger GmbH & Co., KG, Freiburg, Germany) sheet (1 mm in thickness) by a transcaruncular approach under direct endoscopic visualization. Alternatively, a portion of the perpendicular plate of the ethmoid harvested from the septum was used to reconstruct the medial wall.
Postoperative Management
Intravenous methylprednisolone (500 mg) was given daily for 3 days after surgery, in addition to 5 days of intravenous broad spectrum antibiotics. Patients were advised to avoid nose-blowing and strenuous activity for 2 weeks. All patients underwent an endoscopic examination of the ethmoid sinus and the wound surface at 5 to 7 days after surgery. Reviews were carried out at 2 weeks, 1 month, 3 months, 6 months and then as required.
Results
Eight patients were women and 4 were men. The right was involved in 7 patients and the left was involved in 5 patients. The average age was 42.6 ± 12.4 years (range, 22 to 61 years). The most common symptom was a painless, gradually progressive visual decline lasting for an average of 17.8 ± 11.3 months (range, 6 to 38 months). The BCVA ranged from counting fingers at 20 cm to 6/7.5, with significant profound visual field defects. Ten of 12 patients (83%) had a pale optic disc with a relative afferent pupillary defect of the affected eye. No patients had significant exophthalmos, diplopia, or limitation of ocular movement. The Table summarizes the clinical presentation and surgical outcomes of our patients.
| Patient No. | Sex | Age (y) | History (mos) a | Optic Disc | Position of Mass | Surgery | Tumor Size (mm) | BCVA | |
|---|---|---|---|---|---|---|---|---|---|
| Before Surgery | After Surgery | ||||||||
| 1 | F | 42 | 9 | Normal | Superomedial | ETA + IMRM | 20 × 12 | 6/7.5 | 6/6 |
| 2 | F | 35 | 6 | Pale | Optic canal | ETA | 6 × 5 | CF at 20 cm | 6/60 |
| 3 | F | 32 | 11 | Pale | Inferomedial | ETA + IMRM | 12 × 9 | 6/10 | 6/6 |
| 4 | F | 55 | 32 | Pale | Inferomedial | ETA + IMRM | 10 × 7 | 6/24 | 6/12 |
| 5 | F | 41 | 6 | Pale | Superomedial | ETA + IMRM | 13 × 11 | 6/15 | 6/12 |
| 6 | F | 29 | 10 | Pale | Optic canal | ETA | 8 × 4 | 6/30 | 6/20 |
| 7 | M | 61 | 24 | Pale | Superomedial | ETA + IMRM | 17 × 12 | 6/20 | 6/12 |
| 8 | M | 38 | 19 | Pale | Inferomedial | ETA + IMRM | 12 × 6 | 6/15 | 6/10 |
| 9 | F | 22 | 36 | Pale | Inferior | ETA + IMRM | 18 × 11 | 6/15 | 6/10 |
| 10 | F | 45 | 38 | Pale | Medial | ETA | 16 × 14 | CF at 50 cm | CF at 50 cm |
| 11 | M | 50 | 10 | Normal | Inferomedial | ETA | 20 × 12 | 6/10 | 6/7.5 |
| 12 | M | 61 | 12 | Pale | Inferomedial | ETA | 18 × 16 | 6/12 | 6/7.5 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


