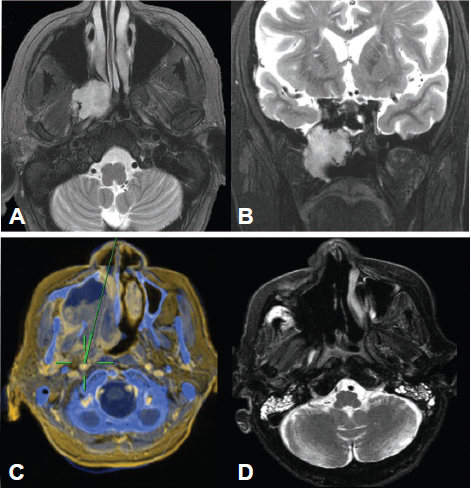
24 Endoscopic Surgery of the Infratemporal and Pterygopalatine Fossae Tumors and lesions of the infratemporal fossa (ITF) and pterygopalatine fossa (PTF) can be addressed surgically through open and endoscopic surgical approaches. Recent experience using expanded endonasal approaches (EEAs) has increased endoscopic access to lesions of the skull base. Although the endonasal “corridor approach” has been well described for midline skull base lesions,1–3 several different endoscopic techniques providing varying degrees of access have been described to access the lateral skull base. These include a trans-septal approach,4,5 a combined Caldwell-Luc/transnasal approach,6 and an endoscopic anterior maxillotomy (EAM) approach.7 Approach selection depends on the anatomic location of surgical target, the type of lesion, the goal of surgery, and the skill set of the surgeon. From an endonasal perspective, the lateral corridor includes any lesion lying lateral to the plane of the medial maxillary wall. Lateral lesions can be located in the medial maxillary wall, the maxillary sinus, or more posteriorly in the lateral sphenoclival bone (vidian nerve), pterygoid fossa, or ITF (Fig. 24.1). Lesions involving the mandibular ramus or arising from the skin or parotid gland lateral to this landmark are best managed through open approaches. More anteriorly positioned lesions of the medial PTF are typically easier to access than those in the lateral and posterior regions of the ITF. Surgical indications include biopsy for histologic diagnosis, surgical debulking, or complete resection. Currently, there are no widely accepted anatomically based staging systems to guide approach selection for lesions of the ITF and PTF. In the authors’ practice, lesions that may be amenable to endoscopic approach include (in order of increasing difficulty) lesions of the medial maxillary wall, the V2 nerve to foramen rotundum, the pterygoid fossa, and the ITF. Approach selection is determined on a case-by-case basis and is defined by the tumor pathology and anatomic location as well as the goal of surgery. Experience and preference of the surgeon are also key factors in approach selection. Successful endoscopic approach to the PTF and ITF requires a detailed anatomic understanding of the region, appropriate instrumentation, and knowledgeable support staff. The surgeon must have enough access to apply effective hemostatic techniques while maintaining an adequate endoscopic view and avoiding inadvertent injury to surrounding structures. The EEA corridor uses a two-surgeon technique to allow three to four hands operating simultaneously. This maintains endoscopic visualization with potential for hemostatic control using a bipolar cautery, endoscopic vascular clip applier, or by packing hemostatic agents. Figure 24.1 Lateral lesions include lesions of the pterygoid fossa and infratemporal fossa. (A, B) Axial and coronal view of schwannoma in pterygoid fossa, abutting the middle cranial fossa through the greater sphenoid wing. (C, D) Squamous cell carcinoma of the maxillary sinus invading the pterygoid fossa and infratemporal fossa. (C) Endoscopic resection revealed positive microscopic margins on the carotid artery (green image-guidance probe). (D) Postoperative imaging 1 year after surgery reveals no recurrence. The patient has no evidence of the disease 5 years after surgery. Careful preoperative analysis of multiplanar imaging helps determine the feasibility of an endonasal approach. There is a wide variation in the degree of aeration of each of the paranasal sinuses and anatomic relations that impacts endoscopic exposure. Review of images in the coronal, axial, and sagittal planes allows an evaluation of the anatomic constraints of an endonasal approach. Multiplanar imaging also provides an understanding of the three-dimensional boundaries of the underlying pathology and surrounding critical structures. Magnetic resonance imaging (MRI) and computed tomography (CT) provide complementary information when evaluating this region: MRI is often helpful in evaluating the soft tissue extent of tumors or lesions, whereas CT imaging provides a detailed view of the bony anatomy. Overlaying them on an intraoperative image-guidance system is useful during surgery. When lesions approximate the carotid artery, magnetic resonance arteriography or CT angiogram can be added for use with image guidance. The PTF is the anatomic space posterior to the maxillary sinus. The PTF extends to the pterygoid plates posteriorly, the posterior wall of the maxillary sinus anteriorly, and opens into the ITF laterally. Vascular structures including the internal maxillary artery and its terminal branches course through the anterior aspect of the PTF, whereas nerves including the vidian nerve, the sphenopalatine ganglion, and the origin of V2 reside in the posterior aspect of the PTF. The PTF can be approached through the posterior maxillary sinus wall. The ITF is an anatomic space below the middle cranial fossa, posterior to the maxilla, and medial to the ramus of the mandible. The ITF must be considered in three planes when considering the optimal approach. The ITF contains both the parapharyngeal space (medially) and the masticator space (laterally). In the axial plane, the parapharyngeal space (PPS) can be divided into pre- and poststyloid compartments. The prestyloid PPS has fewer critical structures, containing primarily fat and an extension of the deep lobe of the parotid gland. The poststyloid PPS contains the internal carotid artery, internal jugular vein, and lower cranial nerves (IX to XII). The medial and lateral pterygoid muscles are located within the masticator space along with the tendon of the temporalis muscle and proximal segment of the internal maxillary artery. The internal maxillary artery courses from a lateral to medial direction and posterior to anterior until it terminates in the pterygoid fossa to form the sphenopalatine artery. The maxillary artery passes lateral to the lateral pterygoid muscle, but it can divide the superior and inferior heads of the muscle and course medial to the inferior head in about 40% of cases.8 The maxillary artery gives several relevant branches within the musculature of the ITF. Notably, the inferior alveolar artery courses medially to the ramus of the mandible laterally, whereas the middle meningeal artery proceeds superiorly, lateral to the V3 nerve. Following the lateral pterygoid plate from anterior to posterior leads directly to the foramen ovale that transmits V3 nerve. This is a safe trajectory of dissection within the pterygoid muscles and extending laterally into the ITF as the carotid artery reliably enters the skull base posterior to foramen ovale. The ITF extends well below the plane of the maxillary sinus floor and nasal cavity floor. This is visualized well on coronal images through this region. Endoscopic access to the inferior aspect of the ITF is quite limited. The variable anatomy of the nasal cavity and paranasal sinuses may impact endonasal access to PTF and ITF lesions. EEAs rely on creating an adequate working corridor to manipulate instruments while maintaining a clear view of the operative field. These approaches typically begin with a wide maxillary antrostomy and total ethmoidectomy. Sphenoidotomy is frequently performed and the middle turbinate may be resected to improve access. The floor and medial wall of the orbit are clearly defined to avoid inadvertent injury. The width of the nasal cavity (determined by the location of the septum and lateral nasal wall and piriform aperture) may compromise mobility of instruments and limit access to the lateral PTF. Septal deviations may be addressed surgically. Removal of the lateral aspect of the medial maxillary wall and inferior turbinate may be required to increase the surgical field, accommodate additional instruments, and improve lateral exposure. A lateral corridor often requires working through the maxillary sinus. The anterior wall of the maxilla transmits the anterior superior alveolar nerves and vessels that supply sensation and blood to the incisors. The posterior wall opens into the pterygoid plates and pterygoid fossa, whereas more laterally it opens into the ITF. The roof of the maxillary sinus forms the orbital floor. Poor pneumatization of the maxillary sinus may compromise access to the superior and lateral regions of the PTF and ITF. The relationship of the maxillary sinus floor with the nasal floor is critical in evaluating endoscopic access to the inferior aspect of the PTF and ITF. A superior position of the hard palate and nasal floor relative to that of the maxillary sinus floor will limit access to the inferior portions of these fossae. The floor of the maxillary sinus descends into the alveolar ridge of the maxilla, below the level of the nasal cavity floor, in about one-third of patients and is at the same level in about one-third of patients.9 The ITF extends significantly below the floor of the maxillary sinus and, even in cases with favorable anatomy, access to inferior aspect of the ITF is limited using an endoscopic approach.
Anatomic Considerations
Pterygopalatine Fossa
Infratemporal Fossa
Nasal Cavity and Paranasal Sinuses
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


