Endoscopic Surgery in the Management of Sinonasal Malignancies
Endoscopic Surgery in the Management of Sinonasal Malignancies
Piero Nicolai
INTRODUCTION
Malignancies of the sinonasal tract are rare, accounting for 3% of all cancers of the head and neck, and present several unique features. Notably, in spite of the widespread use of endoscopy in routine daily practice and progress in imaging techniques, diagnosis is established at an advanced stage in view of the nonspecific symptoms associated with the early phase of growth, which are commonly interpreted as allergy or rhinosinusitis. A second hallmark is the extreme histologic diversity (Table 19.1) that impacts biologic behavior and, consequently, prognosis. In view of their rarity and the lack of prospective comparative studies, most authors can only provide evidence at levels III and IV, and treatment recommendations are based on levels C and D.
The mainstay for treatment of malignancies of the sinonasal tract has traditionally included surgery through an external transfacial approach, followed by adjuvant radiotherapy. From a surgical standpoint, a major step forward in improving the prognosis of tumors with superior extension toward or through the anterior skull base was the introduction in 1963 by Ketcham of anterior craniofacial resection. This procedure has offered previously hopeless patients a possibility of 5-year overall survival of approximately 54%, with, however, a nonnegligible rate of both complications and mortality (33% and 4%, respectively).
Transnasal endoscopic surgery was introduced in the late 1970s as a more physiologic and conservative treatment for sinonasal inflammatory disorders. As a result of the rapidly growing expertise in the field, refinements in imaging diagnosis, and impressive technologic advances in surgical instruments, the indications have expanded to incorporate benign and malignant lesions involving the sinonasal tract and adjacent anatomic areas. The largest experience with malignancies has been accumulated in the management of nasoethmoidal tumors, since for maxillary cancers, external approaches remain the best option.
HISTORY
Unilateral nasal obstruction is the most frequent presenting symptom of sinonasal malignancies, which should always alert the general practitioner and warrant otolaryngologic examination. Other possible associated manifestations are epistaxis, serosanguineous nasal discharge, and impairment of the sense of smell. Orbital signs and symptoms, such as epiphora, dislocation of the globe, diplopia, impairment of visual acuity, and/or movement of the globe, indicate the presence of compression/invasion of the orbital contents. Intracranial extension of the lesion can occur without headache or other neurologic symptoms (Fig. 19.1). The presence of enlarged cervical lymph nodes suggestive of metastasis is an extraordinarily rare event, which is usually seen in high-grade cancers or olfactory neuroblastoma.
PHYSICAL EXAMINATION
Otolaryngologic evaluation in a patient with signs/symptoms suspicious for a nasoethmoidal lesion should include inspection of the face and neck and an endoscopic examination after nasal decongestion. The former aims to identify a swelling in the medial canthal, frontal, or maxillary area; to check the motility of the globes; and to assess sensitivity in the territory of the maxillary nerve. Palpation of the neck, with special reference to levels I-II to disclose any suspicious lymph nodes, is recommended. The advent of rigid and flexible endoscopes has substantially improved the diagnosis of sinonasal diseases. On occasion, the presence of a marked septal deviation can impair visualization of the posterior aspect of the nasal cavity even after decongestion and the use of a flexible endoscope. In this case, it is advisable to explore the nasopharynx through the contralateral nasal fossa to rule out the presence of a mass posteriorly growing through the choana. The most common endoscopic finding in nasoethmoidal malignancies is that of a lesion located lateral or medial to the middle turbinate, varying in color and appearance in relation to the vascularization and the amount of necrosis. In patients complaining of frequent epistaxis, clearly indicating the hypervascularized nature of the lesion, as in olfactory neuroblastoma or melanoma, the inspection must be performed with great caution to avoid any major bleeding. Not infrequently, the lesion completely fills the nasal cavity, so that it is impossible to be certain of the site of origin. In locally advanced lesions, the presence of neoplastic tissue can be observed in both nasal fossae; however, more frequently the nasal septum is simply displaced but not invaded by the tumor.
TABLE 19.1 Histologic Classification of Sinonasal Malignancies (Modified from WHO Classification)
Epithelial Tumors
Adenocarcinoma (intestinal-type and nonintestinal-type adenocarcinoma)
Carcinoma of salivary gland origin
Lymphoepithelial carcinoma
Sinonasal undifferentiated carcinoma
Small cell carcinoma, neuroendocrine type
Squamous cell carcinoma
Soft Tissue Tumors
Angiosarcoma
Fibrosarcoma
Leiomyosarcoma
Malignant fibrous histiocytoma
Malignant peripheral nerve sheath tumors
Tumors of Bone and Cartilage
Chondrosarcoma
Chordoma
Mesenchymal chondrosarcoma
Osteosarcoma
Hematolymphoid Tumors
Neuroectodermal Tumors
Ewing sarcoma
Melanotic neuroectodermal tumor of infancy
Mucosal malignant melanoma
Olfactory neuroblastoma
Primitive neuroectodermal tumor
Germ Cell Tumors
Sinonasal teratocarcinosarcoma
Sinonasal yolk sac tumor (endodermal sinus tumor)
Teratoma with malignant transformation
Secondary Tumors
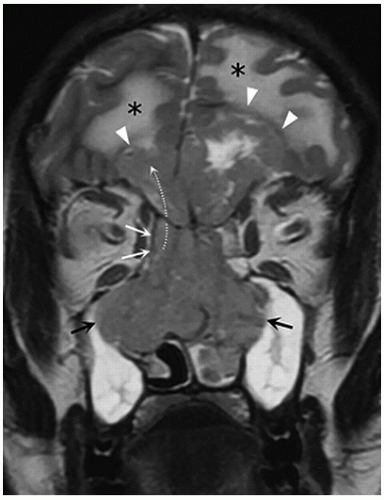
FIGURE 19.1 High-grade nonintestinal-type adenocarcinoma of the right ethmoid sinus in a 45-year-old man, presenting with a 2-month history of bilateral nasal obstruction, with no neurologic symptoms. In the T2-weighted coronal section, the cancer shows intermediate signal intensity, lower than the blocked fluid inside the maxillary sinuses (black arrows). The cancer extends into the left nasal cavity and ethmoid sinus and invades the perpendicular plate. The lesion contacts both the floor and the medial wall of the right orbit (white arrows), without signs of displacement or invasion. Though the low signal of the floor of the anterior cranial fossa can be seen on both sides, the cancer largely extends intracranially through the floor (dotted curved arrow). Cerebral edema (asterisk) surrounds the outline of the intracranial tumor mass (arrowheads). The patient underwent a combined resection (transnasal endoscopic with transfrontal craniotomy) followed by adjuvant radiotherapy.
INDICATIONS
Since the first reports, indications have been to some extent redesigned as a consequence of the increasing surgical expertise and progressive validation of the results obtained. The early experiences included tumors limited to the nasoethmoidal complex and not extending to the anterior skull base, which were managed by endoscopic transnasal resection (ETR). In view of the parallel, increasing expertise acquired in the repair of cerebrospinal fluid (CSF) leaks, it soon became evident that endoscopic resection could be extended to include the anterior skull base with the adjacent dura, olfactory bulb, and tract, mono- or bilaterally according to specific needs (endoscopic transnasal resection with craniectomy, [ETRC]). If the American Joint Committee on Cancer (AJCC) staging system is considered, all T1-T2 and selected T3-T4a-b lesions of the nasoethmoidal complex can be resected through an endoscopic approach.
CONTRAINDICATIONS
The major concern when assessing the feasibility of curative endoscopic resection for sinonasal malignancies is the local extent of the lesion. However, there are situations such as severe comorbidities or the presence of distant metastasis that suggest that the patient is not a good candidate for curative surgery. However, in the latter setting, palliative endoscopic resection may have a role in relieving symptoms such as nasal obstruction or preventing the evolution toward blindness.
Current contraindications in terms of local extent of the lesion for endoscopic resection are summarized in Table 19.2. Erosion of the nasal bones or the floor of the nose, involvement of the maxillary sinus with the exception of the medial wall, invasion of the pterygopalatine fossa, erosion of the pterygoid plates, and involvement of the anterior wall and/or superior aspect of the frontal sinus are all situations that require a combination of an endoscopic with an external approach (otherwise named “endoscopic-assisted external procedure.”) When the lacrimal apparatus or orbital contents are simply compressed or dislocated by the tumor, as is frequently the case in adenocarcinomas, resection can be performed endoscopically, while obvious infiltration requires a combined approach and, after intraoperative histologic confirmation, clearance of the orbit (Fig. 19.2).
TABLE 19.2 Contraindications for Endoscopic Resection of Sinonasal Malignancies
Erosion of the nasal bones or the floor of the nose
Erosion of the pterygoid plates
Extensive involvement of the lacrimal apparatus
Infiltration of the bony walls of the maxillary sinus (except the medial)
Invasion of the orbital contents
Invasion of the pterygopalatine fossa
Involvement of the anterior wall and/or superior aspect of the frontal sinus
Lateral extension of dural resection over the roof of the orbit
Massive involvement of the brain
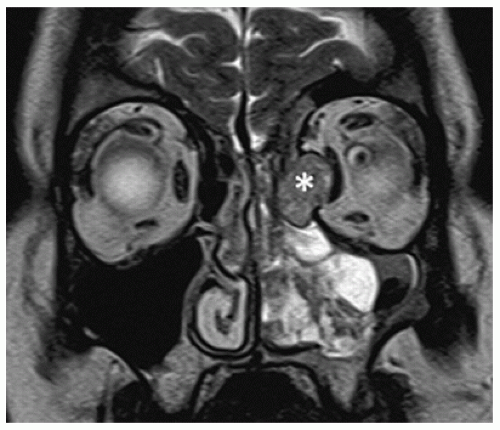
FIGURE 19.2 Inverted papilloma associated with squamous cell carcinoma in a 63-year-old man. T2-weighted coronal plane shows expansile lesion filling the left nasal fossa. Evident orbital infiltration by the solid component directly in contact with the medial rectus muscle (asterisk) can be observed.
In tumors extending to the anterior cranial fossa, a clear limitation for an endoscopic procedure is lateral involvement of the dura beyond the meridian of the orbit, which renders the reconstruction of the dural defect extremely challenging. A second critical issue is involvement of the brain. Apart from any considerations about the prognosis of a patient with involvement of the brain, which is almost invariably ominous, tumors with minimal extension and without major arterial vessel involvement can be easily managed endoscopically, while in all the other advanced situations (Fig. 19.1), resection is more safely accomplished by combining it with a transfrontal craniotomy.
It is also worth mentioning that for some very aggressive histologies (i.e., sinonasal undifferentiated carcinoma, neuroendocrine carcinoma, Ewing sarcoma), which almost invariably present at an advanced local stage, treatment should start with induction chemotherapy to select the next step (surgery or chemoradiation) or directly include chemoradiation. In fact, these tumors tend to have a good response to chemotherapy, which is also used with the intent to prevent early systemic dissemination of the disease. Surgery, irrespective of the technique (endoscopic or combined), plays an important role in the context of multimodality therapy, but not as a first step.
PRETREATMENT PLANNING
The general recommendation when faced with a patient whose symptoms and physical examination are suspicious for a neoplastic lesion of the nasoethmoidal complex is to first perform imaging studies followed by biopsy. Both multislice computed tomography and magnetic resonance (MR) with contrast medium are commonly requested to obtain better delineation of bone and soft tissue extension, respectively. In my experience, MR alone after gadolinium administration and with the acquisition of all the required sequences (Turbo Spin-Echo T2, Spin-Echo T1 pre- and postcontrast agent, Gradient-Echo T1-weighted postcontrast) is accurate enough to obtain the key information for treatment planning (Fig. 19.3):
1. Differentiation of neoplastic tissue from the associated inflammatory modifications within the ethmoid, sphenoid, maxillary, and frontal sinuses
2. Growth of the lesion through the anterior skull base and the periorbita
3. Spread along dura and nerves (i.e., great palatine, vidian, maxillary)
4. Critical relationships with the lacrimal apparatus, optic nerve, internal carotid artery (ICA), and cavernous sinus
5. Involvement of the brain (with or without perilesional edema) and critical contact or encasement of arteries (i.e., orbitofrontal)
6. Erosion of nasal bones or hard palate
Only gold members can continue reading. Log In or Register to continue