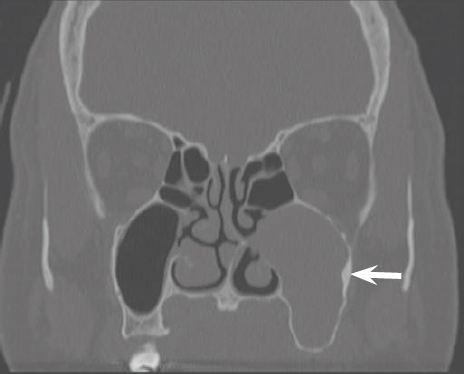
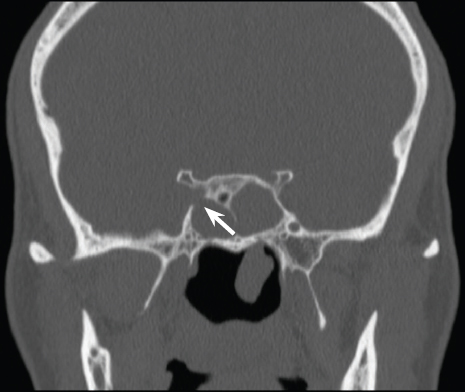
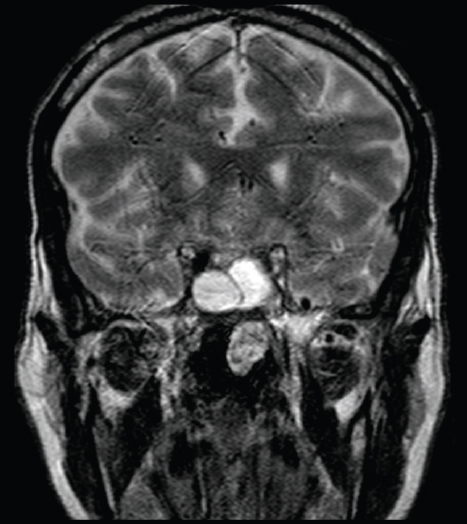
26 Endoscopic Surgery for Inverted Papilloma Inverted papilloma (IP) is one of the most common benign tumors arising from the sinonasal cavity. First described in the 1850s, the surgical management of sinonasal IPs has always been dictated by the tumor’s high recurrence rate and the potential for malignant transformation. To ensure adequate tumor extirpation, open approaches including the Caldwell-Luc, lateral rhinology with medial maxillectomy, and osteoplastic flap have historically been the mainstay of IP surgical management.1–3 With the introduction of endoscopic sinus surgery (ESS) in the mid-1980s, the management of IP has evolved as endoscopic techniques have enabled improved access to the paranasal sinuses and the skull base with reduced patient morbidity.4–6 This chapter aims to review the indications, techniques, and outcomes of endoscopic surgery for sinonasal IP. IPs account for 0.5 to 4.0% of primary nasal tumors with an incidence of 0.2 to 0.7 cases per 100,000 patients per year. They are primarily unilateral tumors but can be bilateral in approximately 5% of cases. The male to female distribution is 3:1 and most commonly present between the fifth and sixth decade of life.3,7,8 Histologically, IPs have their origins from the ectodermal, mucosal lining (Schneiderian membrane) of the nose and paranasal sinuses. They are in fact the most common subtype of the Schneiderian papillomas, with the exophytic fungiform and cylindrical cell comprising the other types. Grossly, they appear as fleshy, gray-tan mucosal lesions that can be more vascular than a typical inflammatory nasal polyp. Histologically, the defining characteristic of the IP is the proliferation of nonkeratinizing squamous epithelium that has an endophytic or inverted growth pattern into the underling stroma. While the stroma may have a variable amount of inflammation, fibrosis, and edema, there is an absence of seromucous glands and the basement membrane is preserved. Typically, IPs have a benign histologic appearance with no significant atypia. Malignant transformation into squamous cell carcinoma (SCC) is a known risk of IP and this rate is often reported to be less than 10%.9 The role of human papillomavirus (HPV) in the pathogenesis of IP has garnered a significant amount of interest over the last several years and remains incompletely defined. In a recent meta-analysis and systematic review, the prevalence of HPV in IP surgical specimens has ranged from 0 to 79%. Overall, the pooled prevalence is approximately 22 to 23% depending on the HPV detection method used. The authors also noted a higher HPV prevalence rate in IPs with dysplasia or malignant transformation.10 The clinical presentation of IP can be quite variable ranging from nasal obstruction, epistaxis, and headaches to the patient being completely asymptomatic. Furthermore, IP can present in the setting of sinusitis and nasal polyps.3,7,8 Given this nonspecific pattern, a high index of suspicion must be maintained to ensure the correct diagnosis and management. Because the tumor is most often unilateral in nature, any patient presenting with unilateral nasal polyps, unilateral sinusitis, or unilateral sinus opacification on imaging should be investigated thoroughly for the possibility of an IP. The most common sites of involvement are typically the lateral nasal wall (89%), maxillary sinus (53.9%), ethmoid sinuses (31.6%), septum (9.9%), frontal sinus (6.5%), and the sphenoid sinus (3.9%).3 One of the most important aspects in the diagnostic work-up of a patient with an IP is imaging. Computed tomography (CT) scans can provide valuable information regarding tumor location and extension by examining the pattern of sinus opacification as well as the integrity of the surrounding bony walls including the orbit and skull base. However, it is often difficult to distinguish between tumor and postobstructive secretions on a CT scan. Recently, it has been found that areas of bony sclerosis or hyperostosis on CT imaging may help identify the site of tumor attachment, an important target during surgical removal (Fig. 26.1). Lee et al in 2007 identified the presence of focal hyperostosis in 48 out of 76 patients with IP. More importantly, these areas of bony thickening identified on CT scan had an 89% positive predictive value for the true tumor surgical attachment, a finding that was corroborated by a similar study performed by Wright et al in 2007.11,12 However, it is important to recognize that these radiologic changes may not be highly specific since bony osteitis is commonly found on CT scans of patients with chronic rhinosinusitis.13 Finally, the role of magnetic resonance imaging (MRI) as a diagnostic modality for IP has also been extensively studied. Karkos et al in 2009 found that T2-weighted images could be helpful in distinguishing tumor from inflammatory tissue. Furthermore, MRIs are particularly useful if there is a suspected tumor extension beyond the bony walls of the sinonasal cavity (Figs. 26.2 and 26.3). However, the utility of the MRI decreases in the setting of recurrent disease as it can be difficult to discriminate IP from scar tissue.14 Ultimately, CT and MRI are complementary imaging modalities in the work-up of patient with suspected IP. The authors experience that the combination of the two is invaluable for preoperative planning. Knowing what inspissated secretions versus solid mass is, it will often be the differentiator between a purely endoscopic procedure and the need for an adjunctive external incision (i.e., trephine) to ensure complete tumor removal. Figure 26.1 Coronal computed tomography scan of a left maxillary sinus inverted papilloma. Note the area of bony hyperostosis on the lateral maxillary sinus wall (a possible area of tumor attachment). Figure 26.2 Coronal computed tomography scan of sphenoid inverted papilloma. Note the bony dehiscence of the right lateral wall overlying the cavernous carotid artery. It is unclear if there is any extension beyond the sphenoid sinus. Figure 26.3 Magnetic resonance image of sphenoid inverted papilloma (same patient as in Figure 26.2). The T2-weighted images demonstrate tumor within the sphenoid sinus but with no invasion of the cavernous sinus or carotid artery. Nasal endoscopy can be of tremendous utility in the diagnosis of IP. In addition to identifying the presence of a nasal mass or polyp, the endoscope may facilitate a biopsy of the suspected tissue under local anesthetic. The role of biopsy for IP has been examined in several studies. In the setting of unilateral nasal polyps, Tritt et al found a 15.9% prevalence rate of IP in patients undergoing ESS.15 However, for bilateral nasal polyps, the prevalence of IP is significantly lower ranging from 0 to 0.92%.16–18 The obvious advantage of a biopsy-proven IP is that it will help in preoperative surgical planning as the extent of surgery will often be different than that for treating inflammatory polyps. This is especially important for patient consent and counseling, particularly if there is any evidence of dysplasia or malignancy. However, clinical biopsies should only be performed if the accessible tissue is not hypervascular and there is clearly no evidence of intracranial extension. The authors’ approach has typically been to attempt a clinic biopsy for suspected IP in patients presenting with a unilateral nasal mass after appropriate imaging has been complete. If the patient is not amenable for a clinic biopsy, a frozen section may be performed at the beginning of the surgical case. For bilateral nasal polyps, we do not routinely conduct clinical biopsies unless the tissue is grossly abnormal on endoscopy. However, bilateral nasal polyp samples are always sent for pathological analysis in all cases of ESS. Table 26.1 Krouse Staging System for Inverted Papilloma
Epidemiology and Histopathology
Presentation and Work-up
Imaging
Nasal Endoscopy and Biopsy
Stage | Appearance |
I | Tumors totally confined to the nasal cavity. |
II | Tumors involving the ostiomeatal complex, ethmoid sinuses, and/or the medial portion of the maxillary sinus (with or without involvement of the nasal cavity). |
III | Tumors involving the lateral, inferior, superior, anterior or posterior walls of the maxillary sinus, the sphenoid sinus, and/or the frontal sinus (with or without stage II criteria). |
IV | Tumors with any extranasal/extrasinus extension to involve adjacent structures such as the orbit, intracranial compartment, or the pterygomaxillary space. Tumors associated with malignancy. |
Adapted from reference 19.
Staging
The Krouse staging system for IP was first described in 2000 and is still the most commonly used (Table 26.1). It attempts to describe the extent of tumor involvement both in the nasal cavity and in the paranasal sinuses. While it is helpful for clinical descriptions of tumor extension, it does not clearly define the indications or limitations of the endoscopic approach for IP tumor removal. Furthermore, while the presence of malignancy (stage IV) is taken into account in this staging system, the issues of tumor attachment and multifocality are not specifically addressed.19 Other staging systems have subsequently been proposed to better reflect the options for endoscopic treatment.20,21 However, these systems are not universally used and are not specifically discussed in this chapter.
Endoscopic Surgery for Inverted Papilloma
The underlying principles of surgery for IP remain the same regardless of whether an endoscopic or open approach is undertaken. Given the high recurrence rate and the possibility of malignant transformation, the goals of surgery should include the following:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


