Endoscopic Sphenoidotomy
The sphenoid sinus is opened in less than 10% of children with sinus disease. The sphenoidotomy can be performed with an ethmoidectomy or alone in the case of isolated sphenoid disease. The safest approach to the sphenoid sinus is through identification of the natural ostium in the sphenoethmoid recess.
24-1 Endoscopic Sphenoidotomy
Indications
Endoscopic sphenoidotomy is indicated for children who remain symptomatic and demonstrate evidence on computed tomography (CT) of sphenoid disease after aggressive medical management with long-term, broad-spectrum antibiotics and topical nasal steroid sprays.
Preoperative Evaluation
Preoperative evaluation includes outpatient anterior rhinoscopy with a telescope or otoscope and CT of the sinuses with coronal views to define the anatomy of the sinuses and extent of sinus disease. The CT should be obtained after a 4- to 6-week course of medical management.
Operative Technique
1. The preliminary steps for endoscopic sinus surgery are performed as described in Section 22-1, steps 1 through 6.
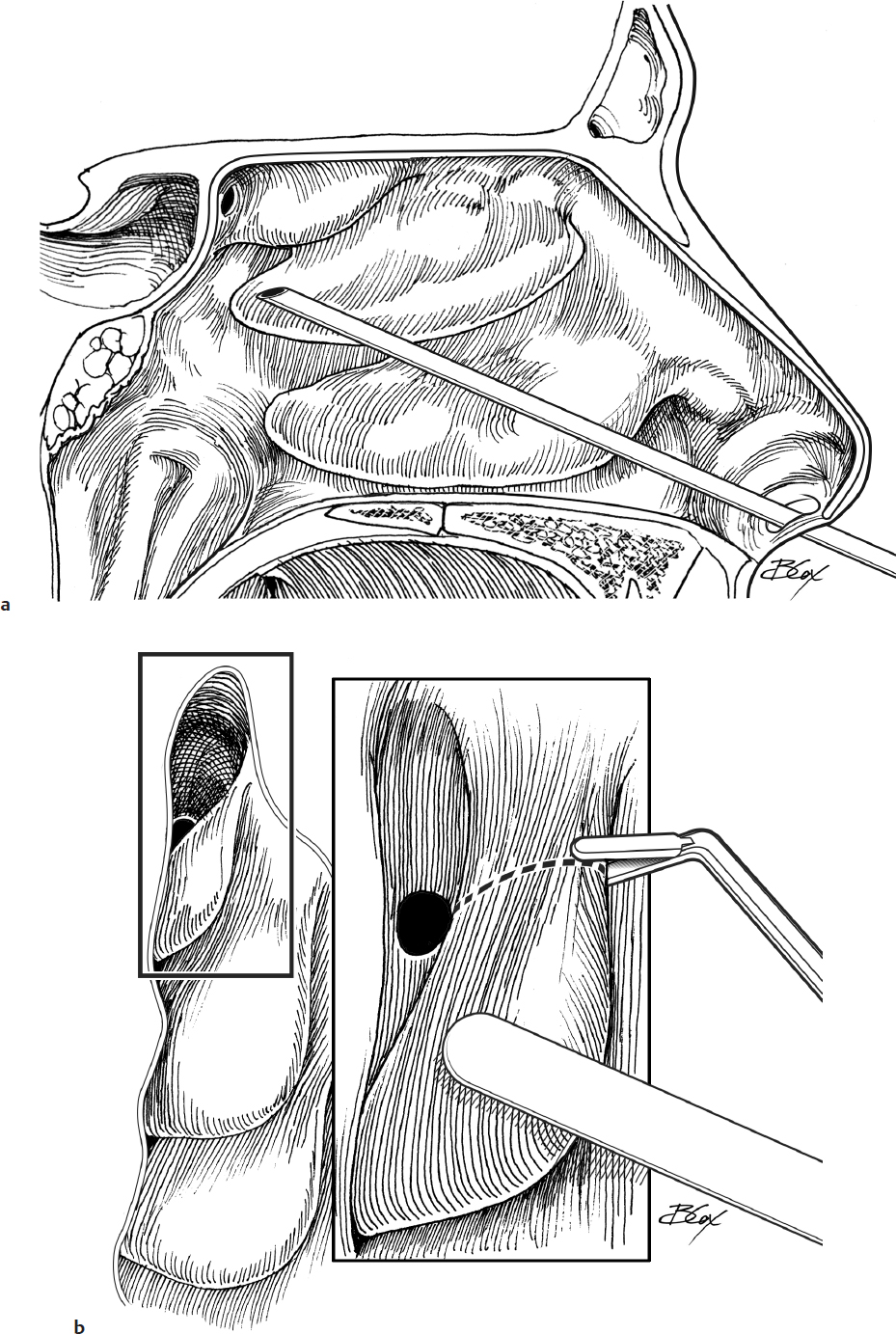
2. For isolated sphenoid sinus disease, the sphenoid ostium can be directly located in the sphenoethmoid recess. First, the superior turbinate in the nasal cavity is identified using a 30- or 45-degree telescope (Fig. 24.1a).
3. The superior turbinate is then lateralized with a Freer elevator to expose the sphenoethmoid recess, which lies medial to this turbinate. If visualization and access are difficult, the inferior half of the superior turbinate is removed with through-cutting instruments or a microdebrider (Fig. 24.1b).
4. The sphenoid ostium can be visualized in the sphenoethmoid recess (Fig. 24.1c). If the ostium is obstructed, it may be located by palpation.
5. Once the ostium is identified, it can be opened using a J-curette directed inferomedially (Fig. 24.1d). The opening can be enlarged with a curette or Stammberger mushroom punch.
6. Mucus or infected fluid can be suctioned from the sinus. Lesions may be removed or biopsied with forceps. Care must be taken to avoid injury to the optic nerve and internal carotid artery, both of which are usually located just lateral to the sinus but may run along the lateral wall to the cavernous sinus.
7. Packing is not usually necessary for an isolated sphenoidotomy.
8. The patient remains on antibiotics, steroids, and saline nasal sprays until seen in the office in 2–3 weeks.
Complications
1. Intracranial complications
a. Cerebrospinal fluid rhinorrhea
b. Intracranial trauma
c. Meningitis
2. Internal carotid artery injury
3. Optic nerve injury
4. Cavernous sinus injury