When the periorbital region is injured with significant force, the bony orbital vault may be fractured. These fractures often involve the medial wall and floor of the orbit, resulting in prolapse of orbital contents into the paranasal sinuses . This may result in extraocular muscle entrapment with diplopia and enophthalmos. Visual loss from optic neuropathy, retinal detachment, or hyphema also may occur. Management of orbital floor fractures traditionally has been accomplished through transconjunctival and subciliary incisions. These approaches provide adequate visualization and cosmetically acceptable scars. Unfortunately, postoperative lid malposition can occur in a small percentage of cases. The most common complications include entropion, ectropion, and lid shortening. Another limitation is easy visibility of the posterior orbit, which often is obscured by prolapsed orbital fat. The introduction of endoscopy and minimally invasive surgery has revolutionized the surgical treatment of many diseases. Endoscopy has become common place in urologic, laparoscopic, and sinus surgery. It offers magnified visualization, access through smaller incisions, less postoperative morbidity, and often greater patient acceptance. This concept now is being evaluated in orbital trauma.
General requirements for endoscopic surgery include the ability to obtain an optical cavity, insert an endoscope, maintain adequate hemostasis, and apply instrumentation. Although several authors have described access to the orbital floor by means of a transnasal approach , complete fracture visualization and reconstruction requires greater access through the maxillary sinus by means of a Caldwell Luc approach. It allows access to the maxillary sinus and excellent visualization of the entire orbital floor, including the stable posterior shelf, which can be difficult to visualize through traditional incisions. Walter described the Caldwell Luc approach for repair of orbital floor fractures in 1972 . His technique involved direct visualization of the fracture with a headlight, blind fracture reduction, and short-term fixation with packing. Since Walter’s description, several authors have described an endoscopic Caldwell Luc approach to orbital floor fractures (Farwell and colleagues, unpublished data, 2004) . This article reviews the indications, technique, and potential complications of endoscopic orbital blow-out fracture repair.
Indications
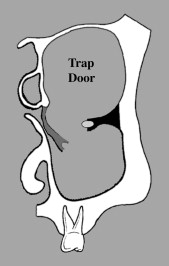
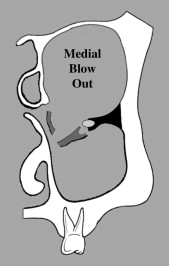
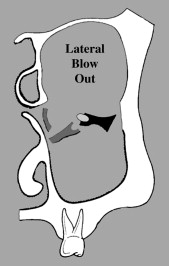
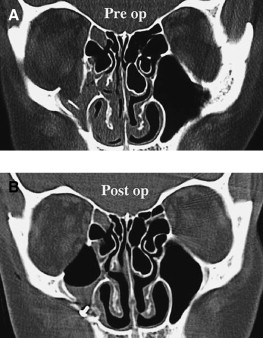
A preoperative CT scan should be obtained to document the location and extent of the orbital floor fracture. Patients with trap door ( Fig. 1 ) and medial blow-out ( Fig. 2 ) fractures are excellent candidates for endoscopic repair. Fractures that extend lateral to the infraorbital nerve ( Fig. 3 ) or involve the lamina papyracea are much more difficult to repair endoscopically and generally require an open approach.
Technique
Under general anesthesia, the patient is placed supine on the operating table. A right-handed surgeon is on the patient’s right side, and the assistant is on the left. The monitor is positioned at the head of the patient, so it can be seen by both surgeons. Two monitors are preferable. Local anesthetic and epinephrine are injected sublabially, and a 4 cm incision is made in the gingivobuccal sulcus, through the periosteum, and onto the maxilla. The periosteum then is elevated, exposing the anterior wall of the maxilla up to the level of the infraorbital nerve. Care is taken to avoid excessive traction on the nerve. An approximate 1.0 cm × 2.0 cm maxillary antrostomy is made in the thin bone of the maxillary face ( Fig. 4 ). This usually is performed with an osteotome and Kerrison rongeur, but the bone can be removed with a saw and replaced after the orbital floor repair. A small notch should be placed along the edge of the antrostomy to stabilize the endoscope and provide tactile feedback for the assistant surgeon. The notch can be placed inferiorly (see Fig. 4 ) or superior-medially depending upon surgeon preference. The lip is retracted with a Greenberg self-retaining retractor, and oxymetazoline-soaked pledgets are placed into the maxillary sinus for decongestion. The orbital floor then is inspected with 0° or 30° sinus endoscopes. The defect is analyzed for size, location, soft tissue prolapse, soft tissue entrapment, and bony comminution. If a trap door injury is encountered with strangulated soft tissue, a small portion of mucosa is stripped away from the fracture. The fracture is opened with an angled retractor, and the orbital contents are reduced into the orbit. The bone flap is then allowed to snap back into place maintaining the reduction. Care must be used to avoid excessive medial dissection that might destabilize the hinge and require placement of an implant.

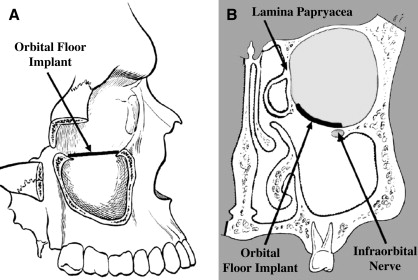
When a medial blow-out fracture is present, the edges of the orbital defect are exposed by conservative elevation of the mucosa around the defect. The entire bony margin must be visualized well. Care must be taken to avoid injury to the maxillary sinus ostia or the infraorbital nerve. The orbital soft tissues then are reduced, and an attempt can be made to reposition the bony piece. More often there is comminution of the floor. In this case, all bone fragments should be removed before reconstruction. When bone is removed, the defect will appear larger, with greater prolapse of the orbital contents. An alloplastic implant (porous polyethylene, 0.85 mm thickness) should be fashioned to recreate the orbital floor and re-establish the orbital volume. The implant should be trimmed to a diameter approximately 1 mm bigger than the defect and inserted through the antrostomy just below the prolapsed orbital contents. Care should be used to assure that no bone fragments are pushed back into the orbital cavity. The implant then is inserted over the stable posterior shelf. A Fraser tip suction catheter and Freer elevator then are used to walk forward on the implant while maintaining the posterior positioning. Gentle force is applied at the anterior portion of the implant (ie, below the posterior aspect of the orbital rim) until it slips over the orbital rim and is stabilized by downward pressure from the orbital contents ( Fig. 5 ). The primary area of support is anterior and posterior. If a medial shelf of bone is present, it can be used also. Pressure laterally on the infraorbital nerve should be avoided.
Once the fracture has been repaired, the endoscope is used to inspect the edges of the fracture looking for any entrapped orbital tissue. A pulse test is performed (ie, gentle external pressure is applied to the globe, and the pulsations are observed through the endoscope) to assure the implant is stable. Forced duction testing is then performed to ensure there is no orbital tissue entrapped during the repair. Any mucosa or bone fragments overhanging the maxillary ostia are removed to minimize the chance of sinus obstruction and subsequent infection. Occasionally, a formal middle meatal antrostomy is required to ensure adequate maxillary sinus drainage. Finally, the wound is closed and a postreduction CT scan is obtained to confirm an adequate repair ( Fig. 6 ).
Technique
Under general anesthesia, the patient is placed supine on the operating table. A right-handed surgeon is on the patient’s right side, and the assistant is on the left. The monitor is positioned at the head of the patient, so it can be seen by both surgeons. Two monitors are preferable. Local anesthetic and epinephrine are injected sublabially, and a 4 cm incision is made in the gingivobuccal sulcus, through the periosteum, and onto the maxilla. The periosteum then is elevated, exposing the anterior wall of the maxilla up to the level of the infraorbital nerve. Care is taken to avoid excessive traction on the nerve. An approximate 1.0 cm × 2.0 cm maxillary antrostomy is made in the thin bone of the maxillary face ( Fig. 4 ). This usually is performed with an osteotome and Kerrison rongeur, but the bone can be removed with a saw and replaced after the orbital floor repair. A small notch should be placed along the edge of the antrostomy to stabilize the endoscope and provide tactile feedback for the assistant surgeon. The notch can be placed inferiorly (see Fig. 4 ) or superior-medially depending upon surgeon preference. The lip is retracted with a Greenberg self-retaining retractor, and oxymetazoline-soaked pledgets are placed into the maxillary sinus for decongestion. The orbital floor then is inspected with 0° or 30° sinus endoscopes. The defect is analyzed for size, location, soft tissue prolapse, soft tissue entrapment, and bony comminution. If a trap door injury is encountered with strangulated soft tissue, a small portion of mucosa is stripped away from the fracture. The fracture is opened with an angled retractor, and the orbital contents are reduced into the orbit. The bone flap is then allowed to snap back into place maintaining the reduction. Care must be used to avoid excessive medial dissection that might destabilize the hinge and require placement of an implant.



