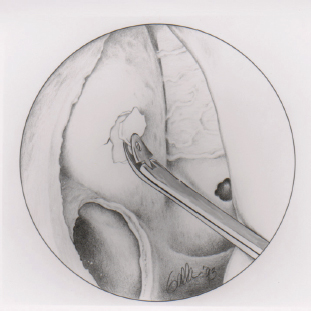
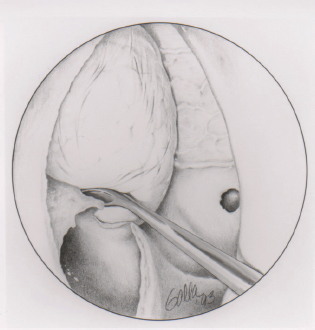
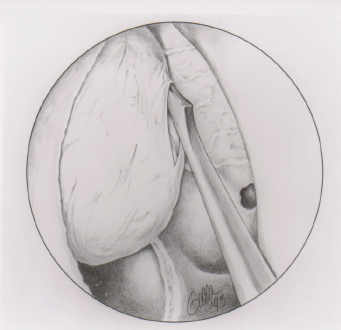
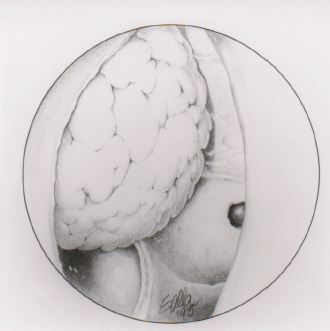
22 Endoscopic Orbital and Optic Nerve Decompression Graves disease is an autoimmune disorder that primarily affects the thyroid and the orbit. Thyroid manifestations are characterized by the production of autoantibodies to the thyroid-stimulating hormone receptor with subsequent hyperstimulation and resultant hyperthyroidism. Orbital manifestations of Graves disease, known as dysthyroid orbitopathy, occur in up to 80% of patients. This represents an autoimmune process, although the exact antibody target remains unclear. Inflammation associated with infiltration of T cells and deposition of glycosaminoglycan results in the enlargement of orbital fat and extraocular muscles. This increase in volume of contents within the confines of the rigid bony orbit results in increased pressure and resultant proptosis, and/or compression of the optic nerve. Clinical manifestations of dysthyroid orbitopathy range from mild findings such as tearing, photophobia, and conjunctival injection to significant proptosis, diplopia, exposure keratopathy, and visual loss from optic neuropathy. The orbital and thyroid manifestations of Graves disease follow distinct and independent clinical courses. Graves orbitopathy is characterized by an initial acute inflammatory phase followed by a chronic, fibrotic phase. The acute phase of orbitopathy typically lasts 6 to18 months and often bears little relation to the degree of thyroid hormone abnormality or its subsequent treatment.1 Local measures such as eye taping and artificial tears are important if corneal exposure is present. During this initial phase, systemic corticosteroids may reduce orbital inflammation and minimize complications. However, because of the side effects of long-term use and frequent recurrence of symptoms following cessation of treatment, steroids are often used as a temporizing measure or in conjunction with surgical decompression. Low-dose irradiation has also been used during the acute phase to counteract the inflammatory process,2 but the efficacy of this controversial modality has been challenged by two recent randomized prospective trials.3,4 Surgery is rarely done during the acute phase unless vision is directly threatened and refractory to nonsurgical treatments.5 Fortunately, severe orbital disease is relatively rare and poses a threat to vision in only 3 to 5% of patients with Graves orbitopathy.6 Eventually, the inflammatory phase gives way to a stable fibrotic phase characterized by statically enlarged extraocular muscles and excess orbital fat. It is during this stable phase, if symptoms persist, that orbital decompression is most commonly performed. Various open decompression techniques involving removal of each of the four walls of the orbit have been described,7–10 with the Walsh-Ogura decompression11 being the favored procedure for most of the 20th century. Initially described in the 1950s, this operation employed the familiar Caldwell-Luc approach to remove the inferior and medial orbital walls, allowing the enlarged orbital fat and muscles to decompress into the ethmoid and maxillary sinus cavities. Soon after the introduction of transnasal endoscopic sinus surgery in the mid-1980s, surgeons began to experiment with endoscopic orbital surgery. Endoscopic orbital decompression was first described by Kennedy et al12 and Michel et al13 in the early 1990s. Enhanced visualization of key anatomic landmarks allowed for safe and thorough decompression of the entire medial orbital wall as well as the medial portion of the orbital floor. This improved visualization is most notable in the region of the orbital apex, a critical area of decompression in patients with optic neuropathy. These advantages have allowed the endoscopic approach to supplant the Walsh-Ogura procedure as the technique of choice for orbital decompression. Initial vasoconstriction of the nasal passages is achieved with topical oxymetazoline (0.05%) or cocaine pledgets. The eyes are maintained within the surgical field and protected with scleral shells. Local injection of lidocaine 1% with 1:100,000 epinephrine is administered along the lateral nasal wall in the region of the maxillary line. The entire medial orbital wall, the medial portion of the orbital floor, and the underlying periorbital fascia are removed during endoscopic decompression. Surgery begins with a complete uncinectomy and maxillary antrostomy. With orbital decompression it is important to widely open the maxillary sinus to achieve adequate access to the orbital floor and prevent blockage of the ostium from orbital fat, which protrudes following decompression. Using a 30-degree endoscope, the wide antrostomy allow easy visualization of the infraorbital nerve as it courses along the floor of the orbit. An endoscopic sphenoethmoidectomy is performed in a standard fashion. We advocate removal of the middle turbi-nate during orbital decompression to optimize exposure of the medial orbital wall and facilitate postoperative cleaning. An image-guidance system may be used at this point to confirm the removal of all ethmoid cells along the medial orbital wall and to ensure complete dissection to the sphenoid face and posterior skull base. Figure 22.1 View of the right nasal cavity during endoscopic orbital decompression. The lamina papyracea is visible along the medial orbital wall with the enlarged maxillary ostium seen below. Once the lamina papyracea has been opened with a small spoon curette, bony fragments are removed with a Blakesley forceps. The skeletonized medial orbital wall is then carefully penetrated with a spoon curette or periosteal elevator. The thin bone of the lamina papyracea is elevated while preserving the underlying periorbita. Bone fragments are removed using Blakesly forceps (Fig. 22.1). Orbital fat should not be visible at this point if the underlying periorbital fascia is left intact. Bone removal proceeds superiorly toward the ethmoid roof, posteriorly to the face of the sphenoid, inferiorly to the orbital floor, and anteriorly to the maxillary line. Bone in the region of the frontal recess drainage pathway is intentionally left intact as herniated orbital fat may obstruct drainage of the frontal sinus resulting in iatrogenic frontal sinusitis or mucocele formation. As dissection proceeds posteriorly, thick bone is encountered in the region of the orbital apex within 2 mm of the sphenoid face. This bone corresponds to the annulus of Zinn, from which four of six extraocular muscles originate and through which the optic nerve passes. This landmark represents the posterior limit of a standard decompression. For patients with optic neuropathy, experienced surgeons may consider continuing the decompression posteriorly into the sphenoid sinus. However, the benefits of incorporating an optic nerve decompression into standard orbital decompression are unclear and the procedure may lead to inadvertent injury to the nerve. Removal of the orbital floor can be technically challenging, depending on its thickness. Only that portion of the floor which is medial to the infraorbital nerve is removed, beginning about 1 cm posterior to the orbital rim. A spoon curette is used to engage the orbital floor along its medial extent and down-fracture the bone (Fig. 22.2). The bone of the orbital floor is thicker than that of the medial orbital wall and significant force may be required for this maneuver. If the spoon curette is not sturdy enough for this portion of the procedure, the heavier mastoid curette may be used. The bone may fracture in one large piece (at a natural cleavage plane along the canal of the infraorbital nerve) or, more frequently, into several small pieces. A 30-degree endoscope and angled forceps may facilitate bone removal while preserving the infraorbital canal as the lateral limit of dissection. Figure 22.2 A spoon curette is used to down-fracture the medial portion of the orbital floor. Once the lamina papyracea and medial orbital floor have been removed, the periorbita is fully exposed. A sickle knife is then used to open this fascial layer (Fig. 22.3). Care must be taken to avoid “burying” the tip of the sickle knife and potentially injuring the underlying orbital contents, including the medial rectus muscle. The periorbital incision should be initiated at the posterior limit of decompression (just anterior to the sphenoid face) and brought anteriorly so that prolapsing fat does not obscure visualization. Parallel incisions are performed along the ethmoid roof and orbital floor. To minimize the risk of postoperative diplopia, a 10-mm wide sling of fascia overlying the medial rectus muscle may be preserved whereas the remainder of the periorbita is removed using angled Blakesley forceps.14 In patients with optic neuropathy or severe proptosis, this fascial sling technique is not used to allow for maximal decompression. A ball-tipped probe and sickle knife may be used to identify and incise remaining fibrous bands that often course superficially between lobules of orbital fat. On completion of the procedure, the surgeon should observe for a generous prolapse of fat into the opened ethmoid and maxillary cavities (Fig. 22.4). Figure 22.3 The exposed periorbital fascia is incised with a sickle knife in a posterior-to-anterior direction. Depending on the clinical scenario and desired degree of decompression, a subsequent lateral decompression may be performed through an external approach that may result in a more balanced decompression. When performed immediately following medial decompression, the orbital contents are easily retracted in a medial direction allowing for excellent exposure of the lateral bony wall. Bilateral decompressions may be performed concurrently or in a staged procedure.
Endoscopic Orbital Decompression
Technique
Printed with permission from: John Wiley & Sons. Metson R, Dallow RL, Shore JW. Endoscopic orbital decompression. Laryngoscope 1994;104(8, pt 1):950–957.
Printed with permission from: John Wiley & Sons. Metson R, Dallow RL, Shore JW. Endoscopic orbital decompression. Laryngoscope 1994;104(8, pt 1):950–957.
Printed with permission from: John Wiley & Sons. Metson R, Dallow RL, Shore JW. Endoscopic orbital decompression. Laryngoscope 1994;104(8, pt 1):950–957.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


