Purpose
To describe the surgical technique for endoscopic medial orbital fat decompression in type 1 (lipogenic) Graves orbitopathy and report outcomes.
Design
Retrospective interventional case review.
Methods
We reviewed 108 patients (206 orbits) with inactive, type 1 Graves orbitopathy without diplopia, who underwent endoscopic medial orbital fat decompression solely for proptosis reduction. Following endoscopic transethmoid medial orbital wall decompression, extraconal and intraconal orbital fat was removed with a low-suction cutting instrument. All patients were followed up for at least 12 months. Surgical time, preoperative and postoperative Hertel exophthalmometry, incidence of postoperative diplopia within 30-degree visual field in the primary gaze, and other complications were analyzed.
Results
The mean surgical time was 97.7 ± 16.7 minutes (67–136 minutes). The mean follow-up was 16.0 ± 4.2 months (12–24 months). Preoperative and postoperative proptosis values at final review were 21.1 ± 2.3 mm (17–26 mm) and 13.0 ± 0.9 mm (12–15 mm), respectively ( P < .001). Median reduction in proptosis was 8.0 mm with mean of 8.2 ± 1.8 mm (4–11 mm). Symmetry to within 2 mm was achieved in 106 of 108 patients (98.1%). Twenty-five of 108 patients (23.1%) had diplopia within 30-degree visual field of the gaze, and 23 of these had complete resolution within 3 months, while the remaining 2 patients required squint surgery.
Conclusions
Endoscopic medial orbital fat decompression may be an effective technique for proptosis in selected patients with type 1 Graves orbitopathy and is associated with a low rate of surgically induced diplopia.
Orbital decompression is a well-established procedure for treating proptosis in Graves orbitopathy, with a variety of techniques including medial, inferomedial, and fat decompression previously described. However, these techniques are at times limited by insufficient proptosis reduction and surgically induced diplopia.
Endoscopic transethmoidal medial orbital wall decompression has become increasingly popular and has been used as an alternative to external approaches. However, it is also relatively limited in the degree of proptosis reduction and orbital floor decompression achievable when compared to traditional techniques. Thus, this approach is often combined with orbital floor decompression or lateral wall decompression. Fat decompression involving excision of both extraconal and intraconal fat through a transconjunctival or transcutaneous eyelid incision has been successfully used to reduce proptosis in Graves orbitopathy, particularly for type 1 orbitopathy (lipogenic variant) compared with type 2 orbitopathy (myogenic variant). However, as a sole procedure, this technique remains limited in proptosis reduction achievable (2.6–6 mm).
We report a new orbital decompression technique involving an endoscopic medial orbital approach enabling bone and fat removal via the nose. A purpose-designed low-suction cutting instrument was developed to facilitate safe, titrated removal of orbital fat. The technique details and outcomes of this procedure are described below.
Patients and Methods
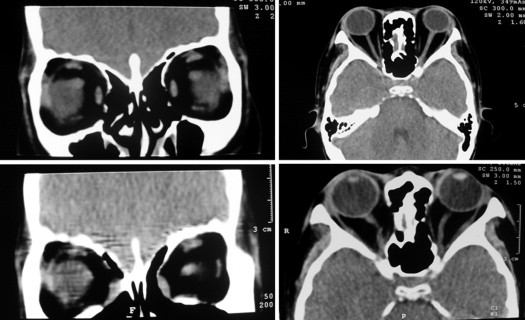
This study was performed at the Eye Hospital of Wenzhou Medical University, Jinhua Center Hospital, Lishui Center Hospital, Quzhou People’s Hospital and Li Huili Hospital, the Second People’s Hospital of Zhengzhou, Xingtai Eye Hospital, and Mianyang Eye Hospital from October 1, 2006 to May 30, 2013, in compliance with the guidelines of the Declaration of Helsinki. Included patients had type 1 Graves orbitopathy ( Figure 1 , Top left) as evidenced by preoperative orbital high-resolution computed tomography (HRCT), showing proptosis secondary to significant expansion of the fat compartment without marked enlargement of extraocular muscles ( Figure 2 , Top left and Top right) and Hertels exophthalmometry measuring >17 mm on 1 or both sides. No patients had preoperative diplopia. All patients had at least a 2-year history of Graves orbitopathy and were in the inactive phase with stable clinical activity scores for at least 6 months, and had been biochemically euthyroid for more than 6 months. Patients with active thyroid eye disease, diplopia, dysthyroid optic neuropathy, corneal ulcers, high myopia (spherical equivalent >6.00 diopters or axial length >26.5 mm 3 ), a previous history of orbital surgery, a previous history of orbital trauma, or unstable thyroid function were excluded. Patients with unilateral proptosis, inadequate medical data, or a follow-up time less than 12 months were also excluded. Additionally, patients who underwent endoscopic medial orbital fat decompression combined with other procedures such as deep lateral wall decompression or orbital floor decompression were excluded. The retrospective review was approved by the local Institutional Review Boards and written consent was obtained from all patients. The surgical procedures were carried out by 3 surgeons (Drs Wencan Wu, Xiaopeng Wang, and Qiao Kong).

All patients underwent orbital examinations pre- and postoperatively, including best-corrected visual acuity, slit-lamp microscopy, biomicroscopic examination of the ocular fundus, Hertel exophthalmometry, and extraocular movements. Exophthalmometry was performed by a single ophthalmologist who was masked to pre- and postoperative state. Diplopia was defined as double vision within a 30-degree visual field in the primary gaze on a Hess chart. All patients were followed up periodically for 12–24 months after surgery. The demographic data; duration of Graves’ orbitopathy; previous treatment history (radioablative iodine/thyroidectomy); values of proptosis, diplopia, and visual acuity; surgical time; and complications were recorded.
All patients underwent preoperative coronal and vertical orbital HRCT ( Figure 2 , Top left and right) and a nasal endoscopic examination. Intravenous methylprednisolone (500 mg) and broad-spectrum antibiotics were administered prior to surgery. No patients were taking antiplatelets or anticoagulation preoperatively.
Surgical Procedure
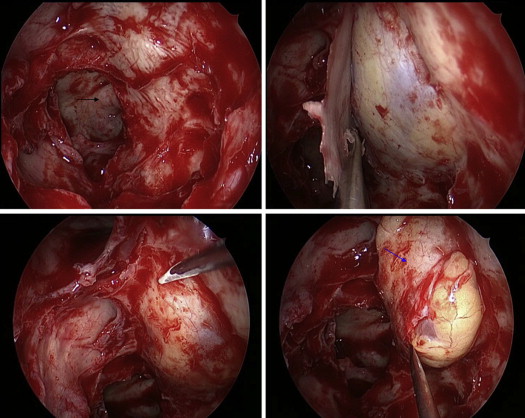
The procedure was carried out under general anesthesia. Nasal vasoconstriction and decongestion was achieved using oxymetazoline-saturated cottonoid pledgets and mucosal injections of 1% lidocaine (1:100 000 epinephrine). Septoplasty was only performed in cases of severe septal deviation. A standard total intranasal endoscopic sphenoethmoidectomy was undertaken as described previously using a 45-degree endoscope (Karl Storz, Tuttlingen, Germany) to expose the posterior medial orbital wall as far as the orbital apex ( Figure 3 , Top left). The lesser wing of sphenoid bone at the orbital apex was thinned using a microdrill (XPS3000; Medtronic Inc, Jacksonville, Florida, USA). The medial orbital wall was dissected off the periorbita ( Figure 3 , Top right) and removed with a microcurette/Freer elevator, as far posteriorly as the junction between the lesser wing of sphenoid bone and the optic canal, anteriorly to the maxillary line, superiorly to the ethmoid roof, and inferiorly to the inferomedial strut between the maxillary sinus and the ethmoid sinus ( Figure 3 , Bottom left). The superior and inferior periorbita was incised from the orbital apex to the maxillary line using a sharp knife to create a band parallel to the medial rectus muscle ( Figure 3 , Bottom right), which was manipulated to extrude orbital fat into the ethmoid sinus.
Endoscopic medial orbital decompression was carried out with a purpose-designed, low-suction cutting instrument (the New Direction Medical Optic Instrument Co, Ltd, Dezhou, PR China) ( Figure 4 ). This instrument consisted of 2 parts: a suction device using a 40–55 mm Hg negative pressure via a suction regulator, and a cutting portion with a sharp edge within the blunt tip, which is operated manually by compressing the handles ( Figure 4 ). The opening of the suction measured 2.5 × 4 mm. A trigger on the handle disengaged the negative aspiration, releasing the fat as required when blood vessels are observed within the fat globules.

A sufficient amount of extraconal fat between the periorbita of the medial wall and the medial rectus muscle was suctioned and removed to expose the inferior edge of the muscle only ( Figure 5 , Top left). The medial rectus muscle was then retracted superomedially using a curved pediatric Lusk ball-probe (Medtronic Inc), enabling exposure and removal of the intraconal fat ( Figure 5 , Top right and Bottom left). Gentle globe compression was used to encourage further fat prolapse. The amount of fat excised was proportional to the reduction in proptosis evaluated by the surgeon; however, the exact amount was not measured.
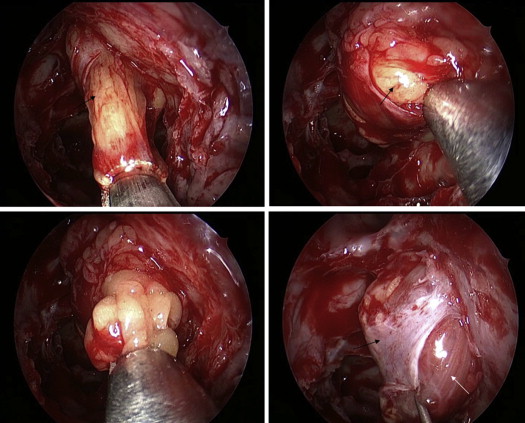
Finally, the middle periosteal band described earlier was repositioned over the medial rectus muscle ( Figure 5 , Bottom right). In the presence of asymmetrical proptosis, endoscopic medial orbital decompression was first performed on the more prominent eye and less fat was then removed from the contralateral orbit to achieve symmetry. Two pieces of Merogel (Medtronic Xomed, Jacksonville, Florida, USA) soaked in antibiotics and dexamethasone were placed to cover the herniated medial orbital soft tissues (Supplemental Video, available at AJO.com ).
Postoperative Management
Intravenous methylprednisolone (500 mg) was given daily for 3 days, in addition to 5 days of broad-spectrum antibiotics. Nasal steroid/decongestants were also used postoperatively. Patients were advised to avoid nose blowing and strenuous activity for 2 weeks. All patients underwent an endoscopic examination of the ethmoid sinus and the wound surface at 5–7 days following surgery. Reviews were carried out at 2 weeks, 1 month, 3 months, 6 months, 12 months, and then as required.
Statistical Analysis
Statistical analysis was performed using paired Student t test to compare preoperative and postoperative values of proptosis. Statistical significance was considered to be P < .05.
Results
From October 1, 2006 to May 30, 2013, 116 Asian patients with type 1 Graves orbitopathy underwent endoscopic medial orbital decompression for proptosis ( Figure 1 , Left). Three patients with unstable thyroid function were excluded, in addition to 3 patients who failed to attend follow-up beyond 6 months postoperatively and 2 patients who did not have Hertel exophthalmometry and diplopia recorded at follow-up review. A total of 108 patients (74 female, 34 male) (216 orbits) were included, with a mean age of 37.6 ± 9.5 years (range 18–57 years). Twenty-one patients had a history of previous thyroidectomy and 42 patients underwent prior radioactive iodine treatment. The mean duration of Graves orbitopathy was 5.5 ± 2.7 years (range 2–20 years). The mean follow-up time was 16.0 ± 4.2 months (range 12–24 months).
The mean surgical time was 97.7 ± 16.7 minutes (67–136 minutes). Pre- and postoperative proptosis values at final review were 21.1 ± 2.3 mm (range 17–26 mm) and 13.0 ± 0.9 mm (range 12–15 mm), respectively ( P < .001). The median proptosis reduction was 8.0 mm and mean reduction was 8.2 ± 1.8 mm (range 4–11 mm). Symmetry to within 2 mm was achieved in 106 of 108 patients (98.1%).
Twenty-five of the 108 patients (23.1%) complained of diplopia within a 30-degree visual field of the gaze in the immediate postoperative phase, of which 23 patients had complete resolution within 3 months. The remaining 2 patients (1.9%) with persistent diplopia were successfully treated with squint surgery.
Nineteen of the 108 patients (17.6%) had epistaxis following surgery, 2 patients developed intraorbital hemorrhages 1 day postoperatively, and orbital emphysema resulted in 3 patients secondary to nose blowing within 5 days postoperatively. All of these cases resolved with conservative treatment. No patients experienced parasthesia postoperatively and there were no cases of medial rectus damage or lagophthalmos.
Results
From October 1, 2006 to May 30, 2013, 116 Asian patients with type 1 Graves orbitopathy underwent endoscopic medial orbital decompression for proptosis ( Figure 1 , Left). Three patients with unstable thyroid function were excluded, in addition to 3 patients who failed to attend follow-up beyond 6 months postoperatively and 2 patients who did not have Hertel exophthalmometry and diplopia recorded at follow-up review. A total of 108 patients (74 female, 34 male) (216 orbits) were included, with a mean age of 37.6 ± 9.5 years (range 18–57 years). Twenty-one patients had a history of previous thyroidectomy and 42 patients underwent prior radioactive iodine treatment. The mean duration of Graves orbitopathy was 5.5 ± 2.7 years (range 2–20 years). The mean follow-up time was 16.0 ± 4.2 months (range 12–24 months).
The mean surgical time was 97.7 ± 16.7 minutes (67–136 minutes). Pre- and postoperative proptosis values at final review were 21.1 ± 2.3 mm (range 17–26 mm) and 13.0 ± 0.9 mm (range 12–15 mm), respectively ( P < .001). The median proptosis reduction was 8.0 mm and mean reduction was 8.2 ± 1.8 mm (range 4–11 mm). Symmetry to within 2 mm was achieved in 106 of 108 patients (98.1%).
Twenty-five of the 108 patients (23.1%) complained of diplopia within a 30-degree visual field of the gaze in the immediate postoperative phase, of which 23 patients had complete resolution within 3 months. The remaining 2 patients (1.9%) with persistent diplopia were successfully treated with squint surgery.
Nineteen of the 108 patients (17.6%) had epistaxis following surgery, 2 patients developed intraorbital hemorrhages 1 day postoperatively, and orbital emphysema resulted in 3 patients secondary to nose blowing within 5 days postoperatively. All of these cases resolved with conservative treatment. No patients experienced parasthesia postoperatively and there were no cases of medial rectus damage or lagophthalmos.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


