Fig. 16.1
Slit-lamp photograph showing (a) white plaque extending from the capsule equator “fluff balls” caused by Aspergillus terreus; (b) retroillumination (Adapted from Al-Mezaine et al. [53])
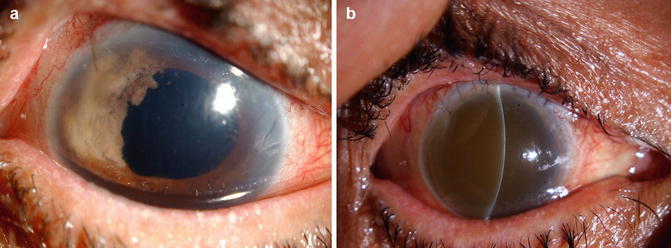
Fig. 16.2
Slit-lamp photograph showing (a) sectoral iris infiltration with Aspergillus niger; (b) fulminant fungal endophthalmitis 2 months later (Adapted from Al-Mezaine et al. [53])
16.4.4 Diagnosis
Diagnosing chronic endophthalmitis poses a challenge. Any intraocular inflammation occurring at any time within several months of a breach of ocular integrity should prompt suspicion of the diagnosis. Anaerobic cultures of intraocular specimens should therefore be monitored for a period of 14 days. However, even after 14 days, these cultures are often negative because most of the organisms are usually sequestered within the capsular bag. Another challenge is the increased likelihood of false-negative culture results owing to the small number of microorganisms in the sample, the physiological requirements of fastidious organisms, and low pathogenicity [75]. Research has shown that PCR is more sensitive than culturing in the detection of chronic endophthalmitis caused by P. acnes [76].
16.4.5 Management
The indolent nature of the organisms and their sequestration within the capsule protects them from host defenses and their different virulence factors make it hard to define a treatment protocol for chronic postoperative endophthalmitis or extrapolate the guidelines set for acute endophthalmitis [70]. Clark et al. [57] and Aldare et al. [58] have proposed several management recommendations: the injection of intravitreal antibiotics alone, followed by PPV with partial capsulectomy, and, lastly, vitrectomy with total capsulotomy and intraocular lens (IOL) removal or exchange.
A cross-sectional review of the biggest case series [53, 57, 59, 77] on chronic endophthalmitis revealed varying results. Differences in causative organism, the type of initial therapeutic method performed, and the extent of the intervention [78] contribute to these varying results. From these series, a total of 98 patients with chronic endophthalmitis were studied. The overall visual outcome was 20/40 or better in about 46 % of the cases, whereas 54 % had varying degrees of visual impairment. An infection caused by P. acnes or gram-positive organisms was associated with a better visual outcome (better than 20/40 in more than 50 % of cases) than an infection caused by other types of bacteria. A fungal infection was associated with a more unfavorable prognosis. Those cases in which the initial treatment involved intravitreal injection alone had the highest rate of recurrence (90 %). The performance of PPV and the administration of intravitreal injections were associated with a decreased rate of recurrence in all series. The inclusion of partial capsulotomy to PPV and the administration of antibiotic injections further decreased the rate of recurrence to 42 % [78]. However, in all series, the overall calculated rate decreased to as low as 50 % when treatment involved PPV, intravitreal antibiotic injections, total capsulotomy, and removal or exchange of the IOL, whereas the rate of recurrence was 68 % when PPV was combined with only intravitreal antibiotic injection [78].
16.5 Posttraumatic Endophthalmitis
Infectious endophthalmitis is a devastating complication of open-globe injuries. It comprises approximately 25–30 % of all cases of infectious endophthalmitis. The incidence of culture-positive endophthalmitis after open-globe injuries varies between 0.5 and 17 % [79–93]. Previous reports have demonstrated that delayed primary repair, dirty wound, breach of lens capsule, retained intraocular foreign body (IOFB), grade 4 injury (presenting visual acuity of worse than 5/200 to light perception), placement of primary intraocular lens, needle injuries, and rural setting are associated with an increased risk of posttraumatic endophthalmitis [79, 81–84, 87, 88, 90–93]. Posttraumatic endophthalmitis is associated with its own microbiologic spectrum which is distinct from other subgroups of exogenous endophthalmitis. Gram-positive organisms such as Bacillus, Staphylococci, and Streptococci are frequently isolated pathogens [79–82, 94–101]. Posttraumatic endophthalmitis still carries a poor prognosis. When pooling data from previously reported studies of posttraumatic endophthalmitis, visual acuities of 20/40 or better were preserved only in 37 % of patients. Reasons for guarded prognosis include polymicrobial infection, the virulence of the infecting microorganisms, and possible delayed diagnosis and initiation of treatment. In addition, concomitant injuries may directly result in ocular damage that limits ultimate visual recovery [79–98, 101].
Useful clinical symptoms and signs in the diagnosis of endophthalmitis after open-globe injury include worsening vision and pain, hypopyon, vitritis, retinitis, periphlebitis, as well as corneal ring infiltrate. Diagnostic imaging in the setting of trauma helps in the detection of suspected IOFB or to rule out retinal and choroidal detachments. Axial computed tomography (CT) scans are most useful for localization of metallic IOFBs. Echography facilitates assessment of the degree of vitreous opacification, presence of IOFB, status of the posterior hyaloids face, as well as detection of either choroidal or retinal detachments.
Because of the substantial incidence of endophthalmitis after open-globe injuries, careful consideration should be given to the use of prophylactic antimicrobial therapy. The purpose of prophylaxis is to provide effective antibiotic level as rapidly as possible against a broad range of organisms. The use of systemic antibiotics in the prophylactic treatment of posttraumatic endophthalmitis has become the standard of care in patients with open-globe injuries, on the basis of clinical experience, but there is little experimental evidence that supports the efficacy of such therapy [79, 82, 95]. Ariyasu et al. [102] demonstrated microbial contamination of the anterior chamber at the time of repair in one-third of their eyes with open-globe injuries. None of these eyes developed clinical endophthalmitis. The incidence of positive anterior chamber culture was significantly lower in patients receiving intravenous antibiotics before wound repair compared with patients not receiving such therapy. These data support the prophylactic use of broad-spectrum intravenous antibiotics against the development of posttraumatic endophthalmitis by reducing the incidence of intraocular microbial contamination. Good coverage for most organisms is obtained with intravenous vancomycin coupled with a third-generation cephalosporin, such as ceftazidime, which can penetrate the vitreous cavity in effective levels in inflamed aphakic experimental eyes [103, 104]. Ceftazidime provides effective coverage for gram-negative intraocular infections [103, 105], and vancomycin provides coverage for gram-positive organisms [104, 105]. The beneficial role of prophylactic intravenous vancomycin coupled with ceftazidime was suggested [90, 92].
Animal models have demonstrated the efficacy of intravitreal antibiotics for prophylaxis of posttraumatic endophthalmitis [106, 107]. A small randomized trial showed that prophylactic intravitreal injection of vancomycin (1 mg) and ceftazidime (2.25 mg) decreases the risk of posttraumatic endophthalmitis [108]. Recently, a multicenter study provided strong evidence supporting the role of adjunct intraocular antibiotic injection at the time of primary repair in reducing the rate of posttraumatic endophthalmitis in open-globe injuries with retained IOFB [109]. Some authors recommended prophylactic intravitreal antibiotic administration in high-risk cases [81, 98, 110]. Therefore, it is crucial to identify these high-risk cases. Essex et al. [88] found that cases with ≥2 of the three risk factors (delay in primary repair of ≥24 h, dirty wound, and lens breach) had a relative risk of 5.1 for developing endophthalmitis. They therefore recommended intravitreal antibiotic injection for these cases at the time of primary repair. In a previous study, we identified clinical risk factors for the development of endophthalmitis after repair of open-globe injuries. Our logistic regression analysis indicated that dirty wound was an independent risk factor for the development of endophthalmitis with a relative risk of 11.6. In addition, the presence of retained IOFB in association with rural address or dirty wound was associated with a high risk for the development of posttraumatic endophthalmitis after primary repair. The relative risks were estimated to be 11.0 and 9.2, respectively, for developing endophthalmitis over those with none of these combinations. We therefore would consider prophylactic intravitreal administration of antibiotics in these high-risk groups at the time of primary repair [92]. The combination of vancomycin (1 mg/0.1 ml) and ceftazidime (2.25 mg/0.1 ml) can be considered in these cases.
Initial treatment of posttraumatic endophthalmitis includes intravitreal antibiotic injection. Directly injecting antibiotics into the globe affords highest drug concentration in the vitreous humor. One must cover gram-positive and gram-negative organisms when treating posttraumatic endophthalmitis. For initial therapy, we recommend intravitreal vancomycin (1 mg/0.1 ml) and ceftazidime (2.25 mg/0.1 ml). In addition to appropriate antibiotic treatment, early therapeutic vitrectomy is often indicated. The use of silicone oil tamponade in vitrectomy for posttraumatic endophthalmitis has been shown to be useful [111, 112].
16.6 Bleb-Associated Endophthalmitis
Bleb-associated infections are infrequent but potentially devastating complication after glaucoma-filtering surgery. The spectrum of disease severity ranges from infection limited to the filtering bleb to intraocular extension leading to endophthalmitis. Blebitis is defined as presumed infection in or around the filtering bleb without vitreous involvement. It may be associated with mild to moderate anterior chamber inflammation.
Bleb-associated endophthalmitis is a devastating complication of glaucoma-filtering surgery. It denotes bleb infection with involvement of the vitreous. The presence of inflammatory cells in the vitreous is a key for differentiating endophthalmitis from blebitis. It usually develops months or years after glaucoma-filtering surgery. Risk factors for its development include the use of an antifibrotic agent, an inferior bleb location, thin bleb, bleb leak, chronic use of antibiotics, blepharitis, prior conjunctivitis and upper respiratory infection, and a history of bleb infection.
The widespread introduction of antiproliferative agents such as 5-fluorouracil and mitomycin-C as an adjunct use in trabeculectomy has remarkably improved the success rate of filtration surgery. However, their use results in formation of thin, avascular blebs, increased risk of late bleb leaks, and a higher incidence of endophthalmitis. Lehmann et al. [113] reported the odds of endophthalmitis to be three times higher in patients who receive antiproliferatives versus those who do not. The reported incidence of bleb-associated endophthalmitis, after glaucoma-filtering procedures with adjunctive mitomycin-C, ranges from 2.1 to 3.2 %. This incidence is higher than the reported rate in eyes undergoing filtering surgery without the use of antifibrotic agents [114–116].
A different microbiological spectrum distinguishes this group from endophthalmitis observed in other clinical settings [114, 117–125]. Unlike acute postoperative endophthalmitis, which results from direct intraoperative inoculation of microorganisms, bleb-associated endophthalmitis follows transconjunctival migration of bacteria into the eye [117]. The poor visual outcome in bleb-associated endophthalmitis could be because of its association with the virulent Streptococcus species and gram-negative bacteria such as Haemophilus influenzae. Exotoxins produced by Streptococcus species might aid the organism in penetrating through intact conjunctiva overlying the bleb. Bleb-associated endophthalmitis is associated with its own microbiologic spectrum which is distinct from that of acute-onset endophthalmitis after cataract surgery. In acute-onset endophthalmitis after cataract surgery, the less virulent coagulase-negative staphylococci, predominantly Staphylococcus epidermidis, was the most common organism, accounting for 70 % of the isolates [105]. On the other hand, the more virulent streptococcal species and gram-negative bacteria such as Haemophilus influenzae are more common causes of delayed-onset bleb-associated endophthalmitis [114, 117–125]. Streptococcal species produce exotoxins and are capable of penetrating the intact conjunctiva overlying the bleb with rapid spread into the anterior chamber and vitreous. The most common isolates are Streptococcus species and gram-negative bacteria, predominantly Haemophilus influenzae, followed by Staphylococcus epidermidis [114, 117–125]. The rate of isolation of Streptococcus species in bleb-associated endophthalmitis is higher than the 9.0 % rate found in endophthalmitis after cataract surgery [105]. Endophthalmitis caused by Streptococcus species was reported to be associated with an aggressive clinical course and a correspondingly poor visual prognosis [126, 127]. Series of bleb-associated endophthalmitis reported that Streptococcus species was the organism most frequently associated with poor visual prognosis [114, 117–122, 124]. These findings are consistent with the results of the Endophthalmitis Vitrectomy Study showing that patients with growth of coagulase-negative Staphylococci achieved the best visual outcome and that Streptococci were associated with the poorest visual outcome [128]. Therefore, the favorable overall visual outcome in patients with endophthalmitis after cataract-related surgery relative to patients with bleb-associated endophthalmitis might be related to the high frequency of infection with coagulase-negative Staphylococci in endophthalmitis after cataract-related surgery [105].
Bleb-associated endophthalmitis still carries a poor prognosis. In combining previously reported studies, visual acuities of 20/400 or better were preserved in only 43 % of patients, and 24 % of patients had final visual acuity of no light perception. Reasons for guarded prognosis include the virulence of infecting organisms [114, 117–122, 124] and ocular comorbidities, such as the advanced stage of glaucoma in many of these patients. However, the poor outcome may also suggest the lack of an effective treatment regimen. In our series we identified a significant association between good visual outcome and better presenting visual acuity, shorter interval from onset of symptoms to treatment, and clear cornea at presentation in the univariate analysis. Shorter interval from onset of symptoms to treatment retained statistical significance in the multivariate analysis. In addition, univariate and multivariate analyses identified diabetes mellitus to be a negative predictor of good visual outcome [124].
Early diagnosis and prompt intensive treatment of blebitis are critical in view of rapid deterioration and potential risk of progression to endophthalmitis, which has relatively devastating outcome. In early stage, conjunctival injection localized to the region of filtering bleb may be noted. Later bleb appears milky, with loss of translucency. Turbid fluid inside bleb may be visible, possibly with frank purulent material in or leaking from the bleb. Inflammatory cells may spill over into the anterior chamber. Hypopyon in the presence of signs of external bleb infection indicates endophthalmitis until proven otherwise. The presence of inflammatory cells within the vitreous is key for differentiating endophthalmitis from blebitis. Slit-lamp biomicroscopy examination of the bleb and Seidel test to detect any bleb leak should be performed. Ultrasound examination of vitreous should be performed if fundus examination is obscured due to inflammation. A swab of conjunctiva over the bleb and an anterior chamber tap should be performed for Gram stain and culture sensitivity before starting antibiotic therapy. Vitreous tap also should be performed if a hypopyon is present or there is any indication of involvement of the vitreous.
Intensive topical broad-spectrum antibiotic regimen alone is appropriate for patients with blebitis, without evidence of vitreous involvement. After the antibiotics have been used for about 24 h and signs of improvement of blebitis become evident, topical steroid should be initiated to prevent scarring and preserve the filtration site. The EVS guidelines for the treatment of post-cataract surgery endophthalmitis [129] cannot be applied to bleb-associated endophthalmitis because it is different in its presentation, infective organisms, and prognosis. Bleb-associated endophthalmitis needs more aggressive treatment. Recent retrospective studies demonstrated that patients treated with initial vitrectomy had better visual outcome and a lower incidence of no light perception vision than those treated with tap and injection [122, 124]. On the other hand, other studies [121, 125] reported worse visual outcome with vitrectomy. In these studies, the patients who underwent initial vitrectomy had a more severe infection and poorer visual acuity at time of endophthalmitis diagnosis. Because of this selection bias, final visual outcomes would be expected to be worse in the vitrectomy group. Compliance with Ethical Requirements Conflict of Interest The authors declare that they have no conflict of interest. Informed Consent No human studies were carried out by the authors for this article. Animal Studies No animal studies were carried out by the authors for this article.
References
1.
Okada AA, Johnson RP, Liles WC, D’Amico DJ, Baker AS. Endogenous bacterial endophthalmitis. Report of a ten-year retrospective study. Ophthalmology. 1994;101(5):832–8.PubMed
3.
Jackson TL, Eykyn SJ, Graham EM, Stanford MR. Endogenous bacterial endophthalmitis: a 17-year prospective series and review of 267 reported cases. Surv Ophthalmol. 2003;48(4):403–23.PubMed
4.
Wong JS, Chan TK, Lee HM, Chee SP. Endogenous bacterial endophthalmitis: an east Asian experience and a reappraisal of a severe ocular affliction. Ophthalmology. 2000;107(8):1483–91.PubMed
5.
Kresloff MS, Castellarin AA, Zarbin MA. Endophthalmitis. Surv Ophthalmol. 1998;43(3):193–224.PubMed
6.
Taban M, Behrens A, Newcomb RL, Nobe MY, Saedi G, Sweet PM, McDonnell PJ. Acute endophthalmitis following cataract surgery; a systematic review of the literature. Arch Ophthalmol. 2005;123:613–20.PubMed
7.
Miller JJ, Scott IU, Flynn Jr HW, Smiddy WE, Newton J, Miller D. Acute-onset endophthalmitis after cataract surgery (2000–2004): incidence, clinical settings, and visual acuity outcomes after treatment. Am J Ophthalmol. 2005;139:983–7.PubMed
8.
Colleaux KM, Hamilton WK. Effect of prophylactic antibiotics and incision type on the incidence of endophthalmitis after cataract surgery. Can J Ophthalmol. 2000;35:373–8.PubMed
9.
Endophthalmitis Vitrectomy Study Group. Results of the Endophthalmitis Vitrectomy Study; a randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Arch Ophthalmol. 1995;113:1479–96.
10.
Maxwell Jr DP, Diamond JG, May DR. Surgical wound defects associated with endophthalmitis. Ophthalmic Surg. 1994;25:157–61.PubMed
11.
Cooper BA, Holekamp NM, Bohigian G, Thompson PA. Case-control study of endophthalmitis after cataract surgery comparing sclera tunnel and clear corneal wounds. Am J Ophthalmol. 2003;136:300–5.PubMed
12.
Nagaki Y, Hayasaka S, Kadoi C, Matsumoto M, Yanagisawa S, Watanabe K, Hayasaka Y, Ikeda N, Sato S, Kataoka Y, Togashi M, Abe T. Bacterial endophthalmitis after small-incision cataract surgery; effect of incision placement and intraocular lens type. J Cataract Refract Surg. 2003;29:20–6.PubMed
13.
Lertsumitkul S, Myers PC, O’Rourke MT, Chandra J. Endophthalmitis in the western Sydney region: a case-control study. Clin Experiment Ophthalmol. 2001;29:400–5.PubMed
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


